Will this work for me, Doc? If only dental teams offering help for sleep-disordered breathing could answer this question with confidence! Will the airway respond to mandibular advancement? How far does it need to move? Where does the airway close? Can we know where the narrowest spot is, and does that information tell us anything? Does the 3D image from a cone beam give us any answers?
Dr. Kent Moore is an oral surgeon in Charlotte, North Carolina with a keen interest in answering these and other questions about imaging the airway with cone beam computed tomography (CBCT). Dental Sleep Practice sat down with Dr. Moore for a take on some of the excitement around this technology.
 DSP: Kent, dentists are either using CBCT or thinking about it: give us an idea about what it is used for in the dental office today.
DSP: Kent, dentists are either using CBCT or thinking about it: give us an idea about what it is used for in the dental office today.
KM: I use mine quite a bit for assessing neurovascular risk prior to implant placement and wisdom teeth extractions; prior to and after any sort of reconstructive facial skeletal surgery, I’ll obtain one. What concerns me is that a lot of dentists are buying these scoped-down versions with limited fields of view, probably for either financial or risk-management reasons. But I don’t want to focus on what might be sales issues – I’d like to talk about what might be coming down the road – then you’ll see why a limited area image may not be helpful. If we think only about what it can tell us about skeletal morphology, they might be missing the point – there can be some real pertinent information in terms of airway size and shape that will hold some utility for us in the future. Today dentists are using scanners for digital impressions for making oral appliances; I think someday the CBCT may have sufficient data and resolution to make the oral appliances directly from this type of scan, but I certainly don’t see the need for digital scanners going away anytime soon.
DSP: Is it the data from the scan that is going to make that available, or is it the software that is improving?
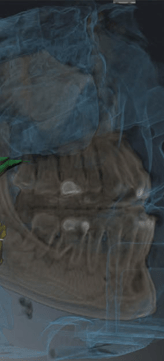
KM: I think it’s both – but I see more software-driven abilities to utilize the data we are getting. There are several good vendors out there offering very good utilities for upper airway assessment. I’m excited, but we do need to take a step back and understand the limitations of cone beam: these scans are being done during wakefulness, while the patient is upright, and they are an average scan over 10, 15 or more seconds with normal tidal breathing going on. You’re going to get an average of the upright wakefulness airway size over the time of the scan, unless the patient is holding their breath. It’s far less radiation than a medical grade scan; getting these average values is one of the trade-offs for that.
 DSP: What does that mean for our ability to diagnose apnea using a cone beam?
DSP: What does that mean for our ability to diagnose apnea using a cone beam?
KM: When you think about it, Obstructive Sleep Apnea is a diagnosis based on a physiologic-based sleep study exam: a sleep study performed in a sleep lab or with a portable monitor while the patient is in a recumbent body position (supine/lateral/prone) during natural sleep. We know that the airway collapses in size from upright wakefulness to supine REM sleep. The cone beam CT Scan, however, produces an image which the doctor examines to study anatomic details typically during upright wakefulness. I don’t think we’re ever going to diagnose apnea purely from an image…particularly one taken during upright wakefulness.
DSP: It seems that most professionals agree that cone beam does a great job of identifying the airway shape, with the limitations you mention, which might indicate risk factors for SDB.
KM: Exactly – with Obstructive Sleep Apnea (OSA) the anatomy predisposes a person to the physiologic problems – small airway size helps us to consider who may suffer from this disease. This will be very powerful as we put airway size and shape together with other measureable factors such as BMI, age, gender, neck circumference, and ethnicity and probably some others which will play into this down the road. What we know now through our current knowledgebase is just not sufficient to predict who will have it and what oral appliances can do to help.
As long as we acknowledge these limitations, I think there are some very exciting things being done with cone beam. The thing that jumps out at me the most right now is incorporating the technology that Dr. John Remmers is introducing. His MATRx device for the first time allows us to titrate the mandibular advancement during sleep to the point that apnea is resolved, at least in a cohort of patients.
If we take that MATRx device, titrate a given patient, and study that patient in both sleep and wakefulness both during the supine and upright positions, we can study how much expansion of the airway has occurred through the use of that device. Specifically, what is the effect on the minimum cross-sectional airway size? We know there is a difference between different-shaped airways, and there have been some published classification systems, by Fujita and one I published in 2002 – which have used endoscopy both while awake and with propofol anesthesia.
I’d like to study patients who have had the MATRx test, not only while they are asleep, but also while they are awake. If we take a baseline scan on a patient and again with the patient in the titrated position, we can go back and compare the airway size at the same point of the anatomy. The working hypothesis is that patients with milder forms of OSA will require less expansion of their minimal airway size (in order to resolve their OSA) as opposed to patients with more severe OSA (who will require greater expansion of their minimal airway size to resolve their OSA).
 If we can gather enough data across a variety of age, gender, ethnicity, BMI and neck size and shape, I really believe we can start to be able to evaluate from a prospective manner who will be a responder to oral appliance therapy.
If we can gather enough data across a variety of age, gender, ethnicity, BMI and neck size and shape, I really believe we can start to be able to evaluate from a prospective manner who will be a responder to oral appliance therapy.
DSP: So will the data that dentists are gathering now be useful to make this prediction?
KM: If we take patients who have had a MATRx test, so we know the position of the mandible in a properly titrated study, that’s very powerful; we can image the mandible at rest and at that titrated point. This could also be done in a MRI during natural sleep – it’s been done at Stanford in a modified MRI. More and more as this type of work progresses, our ability to predict airway response to therapy will improve.
As we can make this data more accessible, even during general upper airway surgery, the surgeon (be it an OMS or ENT) could obtain real-time guidance as to how much to advance the mandible or manipulate the airway during anesthesia to avoid apnea. Taking the next step beyond that, once we know the effective amount of airway expansion needed for a specific demographic of patient, we can use that data to prospectively inform surgeons contemplating corrective jaw surgery or any type of surgical manipulation of the airway — across medical and dental specialities — for that same patient demographic.
Currently maxillofacial surgery for airway improvement is planned using cephalometric data; imagine if the effect on the airway could be known so that the movement could be dictated based upon needed minimal airway size? We’ll need some other data, of course, but I know Sirona has produced a software program named “Function”, which allows a user to see changes in mandibular position during protrusive and vertical mandibular movements. If we can incorporate the airway size data into this program, this would allow us to measure soft tissue response to incremental movement of the bony structures. This could be a very important tool as it becomes possible to link the airway shape to movement. We’re not there yet, but with several software companies working on projects like this, it’s all very exciting.
 DSP: I’ve seen some presentations lately using cone beam data to guide Maxillomandibular advancement surgery planning for airway impact. Instead of guessing, your data might allow the surgeon to be more precise?
DSP: I’ve seen some presentations lately using cone beam data to guide Maxillomandibular advancement surgery planning for airway impact. Instead of guessing, your data might allow the surgeon to be more precise?
KM: That’s exactly what I’m saying. Expanding beyond advancement to any kind of surgery aimed at improving the airway; currently, no one has any way to tell how much airway expansion is required to resolve OSA with any given patient. With the studies I’m proposing, I hope we can crack that nut and be more predictable. The downside is that it’s going to require a lot of studies, carefully done in a statistically valid manner. In this case, by using clinically observable data, we can produce a guideline — using quantitative airway analysis — that everyday doctors can use. Dr. Peter Cistulli, from Sydney, Australia, is probably the world’s foremost researcher in this field; he recently published an elegant article where he constructed an airway model using computational fluid dynamics. This is an incredible feat, but we will still need to perform observational studies looking at varied patient phenotypes.
DSP: So should a dentist contemplating a new imaging device be thinking cone beam rather than another type of digital system? Also, if they are sitting with a patient who seems to be at risk for SDB, should they take a cone beam to assess that risk?
KM: That’s a tough call — right now, for a given set of parameters like the ones I’ve mentioned, we really don’t know what constitutes a ‘small airway’ for any one of these people. Until we have that knowledge base, it’s hard for me to say that screening someone for SDB using a cone beam is legitimate. Although when you consider all the other uses of the image dataset, the ability to see the size of the airway may be important. Dentists buying scanners with a limited field of view may be missing the boat. A limited scanner that doesn’t allow them to image the airway won’t give them any basis for making the call if they can’t compare their patient against norms I hope we will uncover.
I would say if a dentist is interested in sleep medicine and managing patients with oral appliances, there’s no question that’s the investment they need to think about for their practice; I would certainly encourage them to do that. But we still need that sophisticated software, coupled with statistically valid quantitative data — subdivided by patient phenotype — to be able to make the comparisons.
DSP: So the dentist considering making this investment needs to know what capabilities the software may have or be developing to put all these other measurements to use?
KM: That’s exactly right. Having the technology in hand will allow data collection that will build this capability. The way I envision this down the road may be like this: Let’s study a group of Asian males, 30-32 years old, neck circumference of 16.5 inches, and with BMI’s of 28-30, with similar airway shapes who have had a properly titrated MATRx study done. If we can study 100 of these people, we will then have data we can begin prospective studies against. Recruitment will certainly be a challenge, but what I see happening is collecting reference data and using this in a prospective fashion down the road.
 DSP: Could a dentist, trained in what data needs to be collected, participate in a study like this?
DSP: Could a dentist, trained in what data needs to be collected, participate in a study like this?
KM: They could, in fact. I’m in the middle of submitting an application with NIH Small Business Innovation Research for MRI imaging during supine natural sleep, but we’ll need upright, wakeful cone beam data in the study population as well. If we can collect the pertinent demographics and physical metrics into the scanner for each patient and collect the data in a valid manner in a centralized site, we’ll be able to compare. The ethnic component is going to be an important part of this — we see differences between phenotypes but there’s little data. The problems with collecting ethnicity can be solved by using genetic testing with a blood test or even a swab of the cheek. There are companies that can do this testing.
DSP: One question that often comes up is “Should the dentist have the cone beam data read by a radiologist?”
KM: I always have anything suspicious read by a certified orofacial radiologist, but I find that most of them have not done much in the field of airway size assessment. I think if a dentist is looking at a limited use for, say, an implant, there may not be a need for this extra expense — but it is true that if dentists or nonradiologist dental specialists decide to examine their own volumes, however, then they are held to the same standard of care as an oral maxillofacial radiologist and required to find and report any unusual conditions that may reside in that volume. This is a significant responsibility, one that might require additional training for some dentists.
DSP: If we are working with physicians on our sleep patients, though, having a scan read by a specialist is more what they would expect, don’t you think? Does it reduce dentists’ liability for what’s on the scan? Is it worth an extra small cost, which can be billed to medical insurance?
KM: I don’t disagree at all. Any scan interpreted by a certified orofacial radiologist, especially one clued in to airway issues, will help the dentist learn more about the medical aspects of what is being done. This will also help the connection with the sleep docs as they see dentists acting more like medical doctors. It’s going to be a state-by-state issue for dentists’ liability, Steve. You have Dr. Berley writing a legal column for your magazine –that might be a question for him.
DSP: As I mentioned earlier, some companies are overlaying intraoral scanner files with cone beam data and producing virtually articulated images, with the ability to move the mandible according to the anatomy.
KM: I envision a day when that construction, together with a protocol driven by real data about that patient’s airway size, demographic and presenting physical data, can be directed to create an oral appliance to put the patient in just the right position to open the airway. Dr. Remmer’s MATRx device will be a huge step for taking more of the guesswork out of patient care. The thing that really excites me is we have a chance to collect all this data in a HIPAA secure fashion in a central database that will enable us to make a real difference in helping patients. Getting NIH involved, handling my practice, corrective jaw and orthognathic surgery, oral appliances, emergencies in the ER, thinking about what’s next and what’s possible – these are interesting times!
Interview by Steve Carstensen DDS, Editor in Chief
Stay Relevant With Dental Sleep Practice
Join our email list for CE courses and webinars, articles and more..