
Which is better: a kitchen knife or a Swiss Army knife? Each has a sharp blade, but one has many more tools – you can do more than just one action. No matter how hard I try to get people to use the full name “OASYS Oral/Nasal Airway System” it gets shortened to “the OASYS” The “OA” part of OASYS stands for “Oral/Nasal Airway” for the fact that it addresses both the oral and the nasal parts of the respiratory tree, but could stand for “oral appliance”. The important part of the name is “Sys” for System. It is a system for treatment, with multiple functions all working together to get better outcomes for our patients.
 Mandibular repositioning has been established as an effective means of treating obstructive sleep apnea. The many appliances on the market differ only in how they hold the jaw forward. Whether by means of a fin, hook, rod or a strap they all function though the same action, repositioning of the osseous structure of the mandible with the hope that the airway will expand with soft tissue tension. As we shall see, the soft tissue does not always respond to the skeletal movement.
Mandibular repositioning has been established as an effective means of treating obstructive sleep apnea. The many appliances on the market differ only in how they hold the jaw forward. Whether by means of a fin, hook, rod or a strap they all function though the same action, repositioning of the osseous structure of the mandible with the hope that the airway will expand with soft tissue tension. As we shall see, the soft tissue does not always respond to the skeletal movement.

The OASYS stands out from the crowd by adding additional actions and targeting multiple areas of the airway with one convenient appliance. It has two parts: a thin maxillary splint and a fully customized lower active device.
The first goal in designing this appliance was to maximize the intraoral space for the tongue. Using the thin splint on the maxillary arch and a movable shield coming off the lower arch in front of the anterior upper teeth to hold the mandible forward accomplished this. It turned out that the anterior shield feature provides many different health benefits.

Wrench – Easy Slide/Lock
adjustment 8-15mm, forward and
backward, with mm markers.
Optional Lingual Tongue Repositioner
Buttons shown.
The first goal was maximizing tongue space; the second goal being comfort. I knew one of the ways to make the appliances as comfortable as possible was to allow freedom of movement without putting torque on the teeth. Having the main body of the appliance snapping on the lower teeth allows lateral and some up-and-down movement of the jaw without over-stressing the upper or lower teeth. The main force on teeth would be the ‘’pull-back” from repositioning of the mandible, anchored against the upper anterior teeth. The thin upper cushion spreads the force around dental arch.
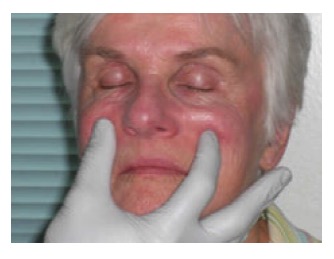
The next insight I had was to reduce nasal resistance, a major issue in sleep disordered breathing that was not being addressed in any appliance. I have experienced the benefit of the Cottle maneuver and wanted to find a way to add this benefit to an oral appliance design. The nasal valve, with internal and external components, is the place where 2/3‘s of the resistance to air flow occurs in the entire respiratory tree.1 The Cottle maneuver 2 is a test that ENT physicians perform by stretching the cheeks laterally, opening the nasal valve to determine if there is improvement in nasal airflow. Through experimenting on myself, a perfect guinea pig, I found that it was possible to mimic the Cottle maneuver intraorally with extensions that stretched the nasiolabial fold. We had the perfect location for the nasal dilators, coming off the anterior upper shield.
The nasal dilators open the nasal valve all night long as well as 27–28% improvement in the middle region of the nasal airway bilaterally with the use of a non-surgical, intra-oral, nasal dilation appliance.
When it came time to obtain a FDA 510K clearance the ENT division of the FDA was brought in and I was asked to show that the nasal dilation was actually caused by the appliance feature. We studied OASYS with and without the nasal dilators in the ENT division of the FDA and our design was officially cleared as a nasal dilator. This is why the OASYS is the only dental device for treating sleep apnea that is cleared in two separate categories, by the dental division of the FDA as a mandibular repositioner to treat sleep apnea and by the ENT division to treat nasal resistance. These findings were published in Sleep and Breathing. 3
With the research that showed exercises such as playing the didgeridoo or doing intensive speech therapy exercises improve the airway and lower the AHI, I started to study tongue anatomy and position in my patients to see if I could understand what was going on and could improve upon the tongue and throat function. These observations revealed many patients with enlarged tongues extending over the occlusal surface, many with scallops on the borders and some that retracted into the back of the throat with the tip of the tongue adjacent to the second molars.
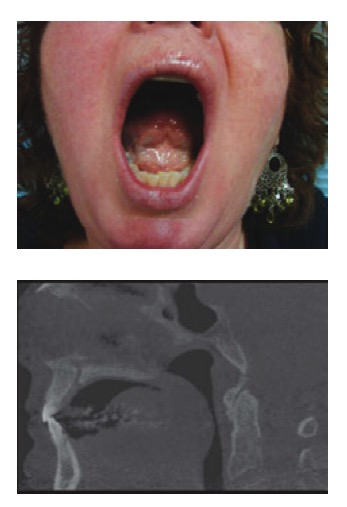
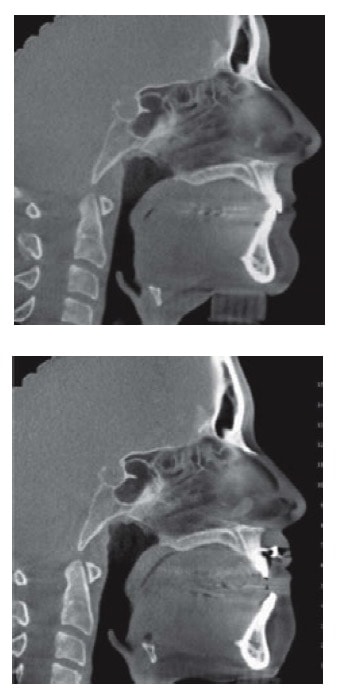
To influence tongue position, I first tried adding a shelf on the entire anterior third of the lower base of the appliance, hoping to lift the tongue up to the palate. What I found was that on many patients that made things worse; instead of the tongue going up over the shelf it would sit behind and be pushed further back into the throat. This is similar to what I observe in patients with large mandibular tori; instead of the tori making the tongue go up to the palate, it would rest behind the tori, pushing the tongue further back into the airway.
I next tried extensions coming off the lower base to guide the tongue up to the palate. This also made the patient’s swallowing more dynamic, establishing a better tongue posture and swallowing pattern.
Instead of discomfort, we have found that the vast majority of patients don’t feel the buttons at all, but they do enjoy the positive effects. I am also working with speech pathologists on a developing a new field I call “Dental Speech Therapy.”
The last benefit is lip closure. Chronic mouth breathing produces a short upper lip; to close the lips together the mentalis muscle pushes the lower lip up to meet the short upper lip. In sleep, the muscle relaxes and lip competency is lost, increasing oral breathing at the expense of nasal breathing. I questioned whether the upper shield would make the situation worse. Fortunately I found that the upper shield had a significant advantage in that even if the lips part, the shield fills the space, sealing the mouth as if the lips are closed. Over time, as recently confirmed by physical therapist Mario Rocabado, the connective tissue in the upper lip stretches and improves lip closure.

In summary the OASYS Oral/Nasal Airway System is a simple, comfortable oral appliance that provides multiple actions addressing the upper airway from the tip of the nose to the back of the throat.