CE Expiration Date: January 30, 2029
CEU (Continuing Education Unit):1 Credit(s)
AGD Code: 730
Educational Aims and Objectives
This self-instructional course for dentists aims to reposition the nose as a clinically meaningful diagnostic organ in dental sleep medicine, by demonstrating how airflow patterns and nasal resistance act as functional biomarkers, and by showing how integrating these measurements can improve intervention planning, therapy tolerance, and patient outcomes.
Expected Outcomes
Dental Sleep Practice subscribers can answer the CE questions online at https://dentalsleeppractice.com/continuing-education/ to earn 2 hours of CE from reading the article. Correctly answering the questions will demonstrate the reader can:
- Describe the multifaceted physiological roles of the nose beyond simple airflow.
- Interpret how nasal airflow patterns and resistance serve as functional “fingerprints” of nasal health and dysfunction.
- Differentiate among airflow states and correlate them with clinical phenotypes in dental sleep patients.
- Apply the concept of “useful resistance” and the Goldilocks Zone to clinical decision-making in dental sleep practice, CPAP/ oral appliance tolerance, and nasal intervention planning.
Karen Parker Davidson delves into how the nose should be treated as a diagnostic organ that affects airflow patterns that can cause sleep issues.

by Karen Parker Davidson, DHA, MSA, MEd, MSN, APRN
Beyond an Airway Passage
The nose is often dismissed as a simple conduit for air, yet its role in health and disease extends far beyond basic anatomy. In reality, the nose is the first diagnostic checkpoint of breathing, a barometer of systemic health, and the gateway to understanding why patients succeed, or fail, in sleep and airway therapies.
For dental sleep medicine providers, this distinction is crucial. When the nose falters, compensatory mechanisms ripple throughout the orofacial complex. In children, this can alter craniofacial growth; in children and adults, it can drive clenching, bruxism, and airway instability; across the lifespan, it perpetuates sleep-disordered breathing and related respiratory disorders.
This article introduces the nose as a diagnostic organ, highlighting how airflow patterns and resistance serve as functional “fingerprints” of nasal health. By reframing nasal function and resistance as measurable, classifiable, and clinically actionable, dental sleep practitioners can better recognize hidden drivers of dysfunction and tailor interventions that restore not just the airway, but also the quality of sleep and systemic health. Think of nasal resistance as the “Fifth Vital Sign”; this is not the first you have heard me propose this concept.
Physiology and Host Defense: The Nose as the First Gateway
Before air reaches the lungs, it must be conditioned, filtered, and regulated by the nasal passages. The nasal turbinates and mucosa create a vast surface area designed for evaporative and conductive heat transfer. Inspired air is warmed toward near-alveolar temperature, humidified to protect the lower airways from dehydration, and filtered to trap particulates and pathogens. Far from trivial, this “air-conditioning” system reduces bronchial reactivity, stabilizes mucosal physiology, and modulates immune signaling to the lungs.
Equally critical is nitric oxide (NO), produced in high concentrations within the paranasal sinuses. Nasal and sinus-derived NO acts as an endogenous antimicrobial, antiviral, and vasoregulatory molecule. It enhances mucociliary clearance, promotes bronchodilation, and directly influences pulmonary gas exchange when inhaled into the lungs. Reduction of nasal NO, whether from chronic rhinosinusitis, polyps, or obstruction, impairs these defenses and has measurable impact on infection risk, ventilatory efficiency, and overall sleep physiology.
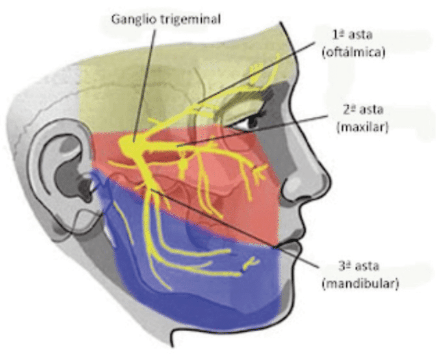
Neuroregulation further underscores the nose’s complexity. Through the trigeminal nerve, the nose communicates with the central nervous system, regulating airflow reflexes, autonomic tone, and even cortical arousal thresholds during sleep. This sensory integration explains why nasal obstruction not only limits airflow but also heightens sympathetic drive, fragments sleep, and increases cardiovascular strain. The nervous system feeds off the nose, and the nose, in turn, feeds off the gut, an emerging concept I coined as the “gut–nose axis.”
Together, these physiological and host-defense functions establish the nose as the indispensable first gateway of sleep breathing, one that cannot be bypassed without consequence to systemic and sleep health.
Airflow Patterns as Diagnostic Signatures
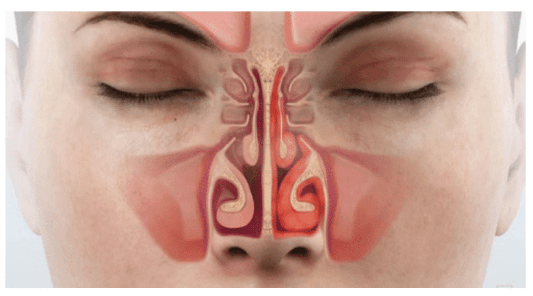
The function of the nose lies in the aerodynamics of respiration. Traditional discussions of nasal obstruction emphasize anatomy; septal deviation, turbinate hypertrophy, and valve collapse, but anatomy tells only part of the story.
Furthermore, resistance in the upper airway is needed to maintain a Functional Reserve Capacity (FRC) of the lungs; we need a certain amount of nasal resistance for optimal function, call it the “Goldilocks Zone” — not too much, not too little, just enough for homeostasis of the airway. This concept was presented as far back as 1973 at the 3rd Congress of the International Rhinologic Society. Since then, computerized rhinomanometric technology has been developed in Germany by Dr. Klaus H. Vogt, an ENT, OMF, and DDS who became frustrated with subjectiveness of his surgical outcomes.1
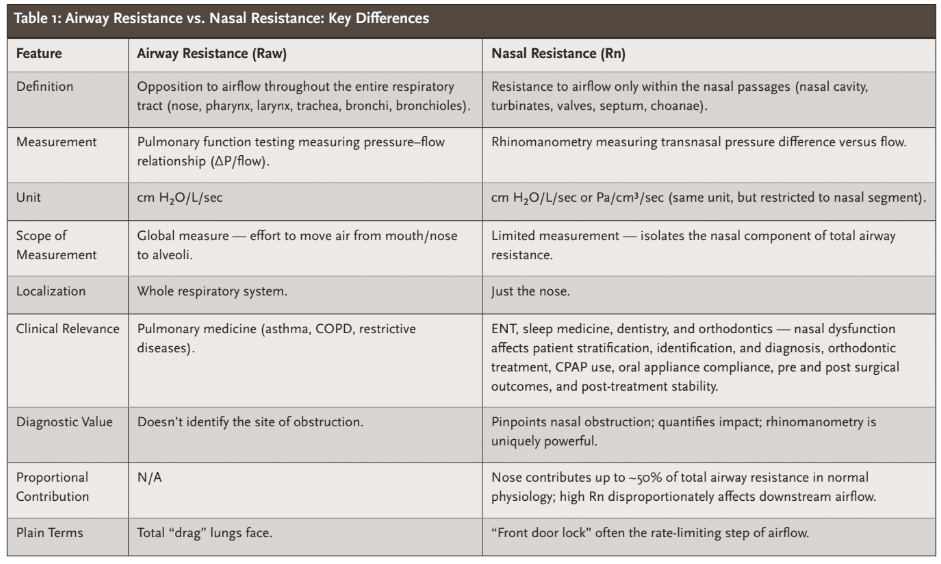
Research from our ENT airway laboratories has since confirmed that the nose is not merely a passive conduit for airflow but an active participant in the aerodynamics of respiration.2-4 In healthy individuals, total airway resistance, distinct from nasal resistance, averages approximately 2.8 cm H2O/L/sec (≈0.275 Pa/cm³/sec), with the nasal passages contributing nearly half of this load (Table 1). This “useful additive resistance” plays a physiological role in stabilizing alveoli against collapse by counterbalancing surface tension forces, thereby supporting functional residual capacity.
Patients with chronic nasal obstruction often leads to adaptive mouth breathing which increases resistance throughout the upper airway and alters respiratory mechanics. Evidence from computational fluid dynamics and clinical sleep studies confirms that nasal obstruction, especially when persistent, raises airway collapsibility and load. For example, in obstructive sleep apnea (OSA) patients, oral breathing is associated with significantly higher resistance and negative static pressures downstream, compared to nasal breathing.
These insights help clarify several long-standing clinical puzzles: why nasal obstruction often feels more pronounced at rest than during exertion; why over-resection of the turbinates can lead to persistent symptoms despite anatomical patency; why some individuals with complete obstruction remain functionally well adapted while others experience significant distress; and why symptoms of Upper Airway Resistance Syndrome (UARS) may recur even after apparent resolution of sleep fragmentation and obstructive nasal breathing through maxillary expansion or nasal bone widening, likely due to a downstream shift in airway resistance known as pseudo UARS (p-UARS) rather than restoration of optimal flow dynamics.1
Modern studies employing computational fluid dynamics and 4-phase rhinomanometry demonstrate that nasal resistance is not inherently detrimental but serves as a key modulator of airflow distribution, lung recruitment, and upper–lower airway integration. The emerging concept of “useful resistance” aligns with contemporary evidence showing that optimal nasal resistance supports ventilatory drive, pulmonary compliance, and even sleep physiology. High-resolution simulations further reveal that it is not resistance itself, but turbulent or unstable flow states, that most often drive pathology. Collectively, this growing body of evidence calls for a fundamental shift in perspective: the nose should be regarded not merely as a passive conduit or site of obstruction, but as a dynamic organ of respiratory regulation and diagnostic significance.
Within this framework, nasal airflow can be classified into distinct categories spanning normal states, resistance-driven flows, pathological dysfunctions, neuroregulated cycles, and extreme disease states. A few illustrative examples:
- Laminar flow: Smooth, efficient airflow with minimal turbulence, seen in healthy noses.
- Turbulent flow: Chaotic, swirling airflow, hallmark of septal deviation or narrowed valves; linked to noisy breathing and snoring.
- Asymmetric partition flow: Unequal right–left distribution (e.g., 70/30 split), often due to deviation or valve collapse.
- Jetting flow: High-velocity streams through narrowed internal nasal valve, perceptible as whistling or localized mucosal trauma.
- Bypass flow: Mouth breathing as compensation, often leading to malocclusion, craniofacial growth disturbance, disturbed oral microbiome, and appliance failure.
- Adaptive flow: A natural fluctuation in nasal resistance that may be exaggerated in disease or reduced in cases of autonomic dysfunction.
- Critical flow limitation: A plateau of inspiratory airflow despite increased effort, mirroring the pathophysiology of obstructive sleep apnea.
Each flow state functions like a diagnostic fingerprint, revealing the underlying drivers of dysfunction: structural, inflammatory, neurologic, developmental, environmental, or systemic. Where a CT scan might show anatomy, and a sleep study might show apnea, airflow analysis connects physiology to clinical outcomes.
The Nose as a Diagnostic Organ: Insights from Resistance Measurements
Nasal resistance is not only a measure of airflow but can serve as a window into systemic health. Thyroid dysfunction, particularly hypothyroidism, may manifest as increased nasal resistance due to mucosal edema, thickened secretions, and decreased neuromuscular tone, narrowing the nasal passages and elevating airflow impedance.5 Similarly, systemic and local conditions such as allergic rhinitis, chronic sinusitis, nasal polyps, asthma, and COPD can alter nasal resistance by influencing mucosal swelling, airway caliber, or bronchial tone.
The gut–nose axis exemplifies shared immune and epithelial barrier mechanisms linking the nasal and intestinal mucosa. Emerging evidence suggests that disruptions in gut health or microbiome balance, through dysbiosis or systemic inflammation, can manifest in the nose as mucosal edema, congestion, and increased resistance.6,7 These changes may worsen breathing difficulty, sleep fragmentation, or CPAP intolerance. This highlights the nose as a sensitive organ that reflects broader systemic and mucosal health, extending its diagnostic value beyond local structural factors.
Pharmacologic influences are equally revealing: antihistamines, decongestants, and corticosteroids tend to reduce nasal resistance by mitigating inflammation, whereas beta-blockers or sedatives may increase resistance by diminishing neuromuscular tone.8-10 Accordingly, careful measurement of nasal resistance can alert clinicians to metabolic disturbances or the physiologic impact of medications, positioning the nose positioning the nose as a sensitive, signaling organ that reflects broader systemic or pharmacologic influences.
Why the Nose Matters in Dental Sleep Practice
For dental sleep medicine, nasal function is not peripheral, it is foundational. Several domains illustrate why:
- Nasal Dysfunction Drives Mouth Breathing: When resistance rises, patients shift to oral breathing. This compensation alters jaw posture, tongue position, and craniofacial growth. In children, mouth breathing promotes long-face syndrome, high-arched palates, and malocclusion. In adults, it perpetuates clenching, bruxism, TMJ strain, and reduced appliance efficacy, and impacts oral health.
- Nasal Resistance Predicts Therapy Success and Stability of Outcomes: Oral appliance tolerance, CPAP adherence, and even surgical outcomes correlate strongly with nasal resistance. Patients with unresolved turbulent or jetting flow often fail CPAP due to discomfort, leak, or intolerance. Similarly, oral appliances are less effective when nasal obstruction forces persistent mouth breathing.
- Diagnostic Potential Across Systems: Airflow patterns reflect not just local
obstruction but systemic disease. Congested flow may signal allergic or infectious inflammation; paradoxical or oscillatory flows may point toward neurologic dysregulation; critical flow limitation highlights overlap with OSA physiology. Recognizing these patterns allows dentists to identify when referral, co-management, or airway testing is warranted. - Objective Testing Validates Clinical Insight: Tools such as 4-phase rhinomanometry and Peak Nasal Inspiratory Flow (PNIF) meter rhinometry allow for measurement of resistance, partition flow, and pressure responses in the nasal cavity. When paired with clinical exam and patient-reported symptoms, they transform subjective impressions into objective diagnostics, bridging dental, medical, and sleep disciplines.
In sleep-disordered breathing, the difference between laminar and turbulent airflow may determine whether therapy succeeds or fails.
Case Vignettes: Airflow in Action
- Case 1 — Appliance Intolerance: A 48-year-old male with OSA failed oral appliance therapy due to persistent mouth breathing. Rhinomanometry revealed asymmetric partition flow (80/20), consistent with nasal valve collapse. After valve repair, appliance tolerance and AHI improved significantly.
- Case 2 — Pediatric Malocclusion: A 10-year-old girl presented with high-arched palate and crossbite. Evaluation showed chronic bypass flow (mouth breathing) driven by adenoid hypertrophy and turbinate enlargement. Adenoidectomy and orthodontic expansion restored nasal breathing, stabilizing dentofacial growth.
- Case 3 — CPAP Intolerance: A 55-year-old female discontinued CPAP due to “air leak.” Testing revealed turbulent expiratory airflow through narrowed nasal valves and concurrent hypothyroidism. After septoplasty with turbinate reduction and levothyroxine adjustment, CPAP tolerance improved, adherence increased, and symptoms resolved.
These cases highlight how recognizing airflow patterns can change the trajectory of treatment.
The Nose as a Roadmap for Airway Care
For too long, nasal evaluation has been relegated to the ENT clinic, considered peripheral to dentistry, orthodontics, and sleep medicine. But the evidence is clear: the nose is the diagnostic compass of airway health. Its flow patterns and resistance provide real-time, physiologic insight into why patients mouth breathe, fail therapy, or relapse after orthodontic treatment.
For dental sleep practitioners, adopting a nasal-centric lens means:
- Expanding differential diagnosis beyond the oropharynx.
- Identifying hidden barriers to appliance and CPAP success.
- Recognizing systemic and neurologic contributions to airway disease.
- Partnering in multidisciplinary care with ENT, pulmonology, pediatrics, and sleep medicine.
As sleep-disordered breathing continues to challenge patients and providers alike, the opportunity lies not in adding more appliances or machines, but in re-centering on the body’s own diagnostic gateway.
The nose is not just the first step of breathing, it is the roadmap to understanding airflow, function, and ultimately, the success of sleep and dental airway care.
Breathing properly through the nose can help athletes compete at their best. Read “The Athlete’s Secret Ingredient: The Power of Nasal Breathing,” here: https://dentalsleeppractice.com/the-athletes-secret-ingredient-the-power-of-nasal-breathing/.
References
- Parker Davidson K. Breathe Through Your Nose, Don’t Pay Through It: The Impact the Healthcare Industry Has on Nasal Function and How We Breathe. 1st ed. PeeDee Publishing; 2022. Revised ed. 2024.
- Bauer SM, Vog K, Wernecke KD, Rasp, Davidson KP, Roesch S. Quantitative measurement of the flow depending nasal valve function by elastography with electro-optical distance sensors. A pilot study. Journal of Biomechanics. Published online 14 September 2024, 112326. https://doi.org/10.1016/j.jbiomech.2024.112326
- Vogt K, Parker-Davidson K. Measurement of nasal obstruction: rhinomanometry as basic method in functional rhinology. Facial Plast Surg. Published online January 15, 2024. doi:10.1055/a-2218-5883
- Bauer SM, Vogt K, Wernecke KD, Rasp G, Davidson KP, Roesch S. Elastometry – The biomechanical analysis of the lateral nasal wall. J Mech Behav Biomed Mater. 2024;150:106284. doi:10.1016/j.jmbbm.2023.106284
- U P S, Kuruwatti A, Nasser A. Relationship Between Rhinitis, Nasal Obstruction and Hypothyroidism: A Follow Up Study with Pre-post Treatment with Levothyroxine. Indian J Otolaryngol Head Neck Surg. 2023;75(3):1394-1398. doi:10.1007/s12070-023-03547-1
- Chandra RK, Lin D, Tan B, et al. Chronic rhinosinusitis in the setting of other chronic inflammatory diseases. Am J Otolaryngol. 2011;32(5):388-391. doi:10.1016/j.amjoto.2010.07.013
- Book DT, Smith TL, McNamar JP, Saeian K, Binion DG, Toohill RJ. Chronic sinonasal disease in patients with inflammatory bowel disease. Am J Rhinol. 2003;17(2):87-90.
- Daley-Yates PT, Larenas-Linnemann D, Bhargave C, Verma M. Intranasal Corticosteroids: Topical Potency, Systemic Activity and Therapeutic Index. J Asthma Allergy. 2021;14:1093-1104. Published 2021 Sep 8. doi:10.2147/JAA.S321332
- Alromaih S, Alsagaf L, Aloraini N, et al. Drug-Induced Rhinitis: Narrative Review. Ear, Nose & Throat Journal. 2022;104(9):582-590. doi:10.1177/01455613221141214
- Cingi C, Ozdoganoglu T, Songu M. Nasal obstruction as a drug side effect. Therapeutic Advances in Respiratory Disease. 2011;5(3):175-182. doi:10.1177/1753465811403348