Dr. Maria Sokolina talks about how dental sleep clinicians can offer OSA patients in clear aligner therapy the option of the Aligner Sleep Appliance (ASA) for maintaining proper breathing.
 by Maria Sokolina, DDS, D.ABDSM
by Maria Sokolina, DDS, D.ABDSM
A lot of obstructive sleep apnea (OSA) patients have misaligned, crowded teeth that impinge on the tongue space, forcing the tongue into the airway. An Aligner Sleep Appliance in combination with Clear Aligners can address the misalignment of the teeth and achieve restorative goals after orthodontic therapy. Patients can use the ASA with modified clear aligners during restorative treatment as well.
An Aligner Sleep Appliance in combination with Clear Aligners can be a useful solution for practitioners who are preparing their patients for orthognathic surgery to correct OSA. Most patients who seek orthognathic surgery have misaligned teeth and are also seeking surgery because they could not tolerate CPAP therapy.
Abstract
Patients that present with obstructive sleep apnea (OSA) often have co-existing dental conditions including bruxism and dental malocclusions1-3 (Figures 1-5). Comprehensive treatment for these patients requires customized plans that take into account individual anatomy, medical history, lifestyle, and preferences. This report details one such case in which we were able to significantly improve a patient’s sleep and breathing quality with a combination of oral appliance, clear aligners therapy, myofunctional therapy, and home remedies to relieve nasal congestion.

Introduction
An estimated 2-4% of middle-aged Americans meet the diagnostic criteria for obstructive sleep apnea (OSA), with up to a quarter of men between 30 and 49 years of age potentially experiencing sleep-disordered breathing.4 The gold standard treatment for OSA is continuous positive airway pressure (CPAP) therapy, but adherence to CPAP therapy is low.5 Mandibular advancement devices (MAD) are a common alternative for patients who do not want to use or do not tolerate CPAP therapy. These devices increase space in the airway by repositioning the lower jaw forward to create more room for the tongue. However, the majority of patients with OSA have dental pathologies, including dental problems such as dental malocclusion, teeth crowding, and loss of tooth structure due to bruxism.1-3 These coexisting conditions can complicate the treatment of OSA, even as treatment of them can decrease the severity of OSA.6 Traditionally, the treatment of dental malocclusion requires the use of CPAP therapy while the patient is undergoing Clear Aligner treatment. This can pose a significant obstacle, as Clear Aligner treatment typically takes 19-24 months.
Here, we describe a case where a patient presented with OSA and CPAP intolerance, as well as bruxism and dental malocclusion. Comprehensive treatment required a multi-disciplinary approach including oral appliances, orthodontic treatment, myofunctional therapy and nasal saline irrigation.
Report of Case
A 60-year-old male was referred to our practice due to CPAP intolerance. His chief complaints were dry mouth, air in the stomach, and dry eyes from the CPAP machine. Patient used nasal pillows and a full face mask during his 3 years of CPAP therapy. The patient has a history of high blood pressure, nasal congestion and chronic sinus infections and moderate OSA. Patient complained of a dry mouth in the morning with or without a CPAP machine. He was informed by his bed partner that he kept his mouth open during his sleep and for that reason he kept a glass of water next to his bed during the night.
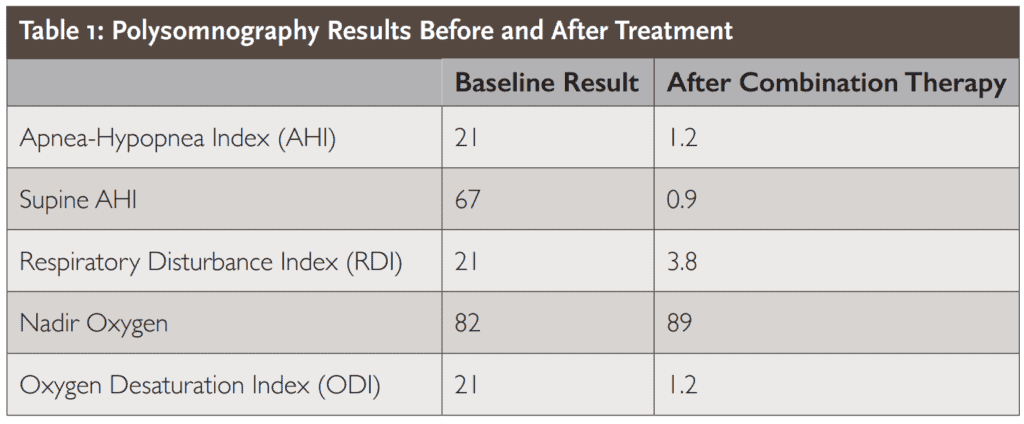
Oral examination revealed upper and lower dental crowding and bruxism. The results of the initial polysomnography are presented in Table 1. Upon consultation, the patient expressed the desire to correct the malocclusion and address the loss of tooth structure due to bruxism.
While we were discussing treatment options, I mentioned that surgery could be a viable choice to eliminate my patient’s OSA, once they have fully recovered from the procedure. However, he ultimately decided to prioritize addressing his aesthetic concerns.
The patient was offered two treatment options. The first plan included using a dorsal oral appliance to protrude the lower jaw and tongue forward, which would help increase the size of the airway’s lateral dimension. That solution only addresses breathing problems while leaving the underlying dental pathology intact.
The alternative plan was a more comprehensive approach. It included: (1) a referral to a myofunctional therapist to improve tone and function of the tongue, promote nasal breathing, create lip competency (2) clear aligner therapy (Invisalign) in combination with the Aligner Sleep Appliance® (ASA; SleepArchiTx, Newport Beach, CA). Clear aligner therapy would help correct crowding and expand the dental arches, while the ASA would assist in both dental arch expansion and protruding the lower jaw and tongue forward, ultimately increasing the size of the airway’s lateral dimension, (3) Restorations of loss tooth structure due to bruxism with Zirconia veneers. The patient chose the alternative treatment plan as prescribed.
The goals of the myofunctional therapy sessions were to train the patient to: (1) create direct contact between the tongue and palate; (2) be able to hold his tongue in a flat position on the palate; (3) move his tongue independently from his lower jaw, (4) keep lips together during day and night; and (5) promote nose breathing during day and night.
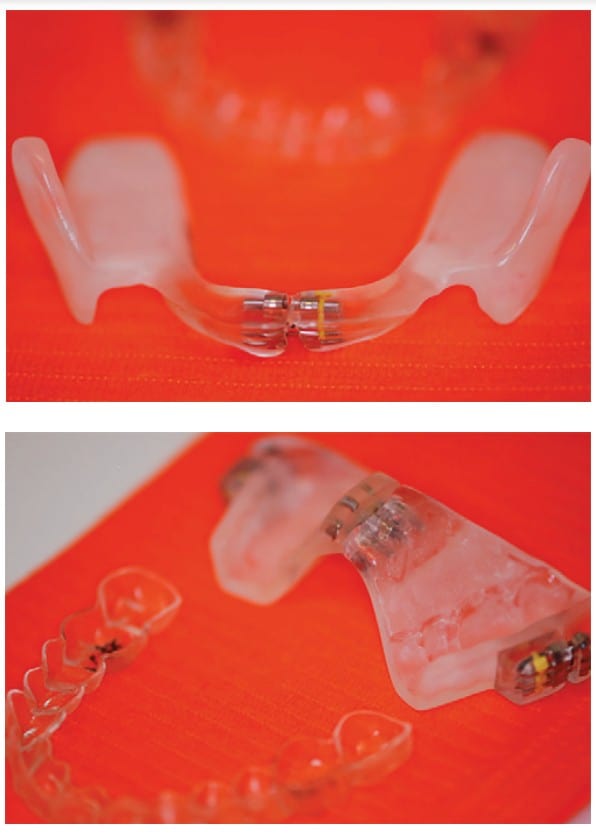
For the oral appliances, the patient was instructed to wear custom clear aligners 20-22 hours a day and the ASA every night on top of the clear aligners. Treatment for clear aligners and ASA started at the same time (Figures 6-7). Patient had prescribed 20 aligners for the upper arch and 22 aligners for the lower arch. In addition to the protrusion mechanism, ASA has a 5 mm expansion screw to accommodate the expansion with clear aligners. He had a positioner made to use over the clear aligners to reposition his jaw in the morning and was instructed on the hygienic maintenance of all oral devices (Figures 8-10). The patient changed clear aligners every 10 days and monitored the amount of time he was wearing the clear aligners during the day with the TrayMinder Invisalign Tracker app.

The patient received additional home remedy suggestions to prepare him for successful adaptation to ASA therapy. First, the importance of nasal breathing was discussed. Second, the patient was advised to rinse his nose with saline in the morning and evening using the NeilMed sinus rinse squeeze bottle system. Third, the patient was instructed to use tape over the mouth to promote nasal breathing at night. Finally, the patient was asked to use the SnoreLab app on his phone to record his breathing sounds during sleep before and during the course of treatment.
The patient reported rinsing his nose with saline before going to sleep significantly helped with nasal congestion at night. However, he reported anxiety over taping his lips at night. It was recommended that he begin by taping his lips for 5 minutes during the day to promote nasal breathing and increasing the duration over time.
The patient adapted easily to the combination clear aligner and ASA therapy. After the original insertion, he reported immediate side effects of increased salivation and slight discomfort of dentition, which were addressed in a follow-up phone call. Patient had his ASA advanced 4 mm horizontally and 2 mm transverse during the first 3 months. The patient got through 17 out of 20 clear aligners before the aligners stopped tracking his teeth according to clear aligner therapy standards. The ASA reached a maximum expansion of 5 mm and became less stable due to the full opening of the screw. Therefore, new refinement aligners and a new ASA were ordered after 6 months of treatment. Patient received 22 upper aligners, 18 lower aligners and started the refinement stage with a new ASA appliance. During the treatment plan financial presentation, we discussed the possibility of refining the treatment with clear aligners and ordering a new version of the Aligner Sleep Appliance (ASA) to continue with the expansion of the arches. We explained to the patient that creating space between the anterior teeth would require minimal preparation for Zirconia veneers. This required a new ASA with a new expansion screw to accommodate the existing expansion and achieve an additional 5 millimeters.
The patient filled out the Epworth Sleepiness and Fatigue Scales at each appointment,8,9 and reported that his snoring was significantly reduced. Tiredness and sleepiness improved. On the SnoreLab app, the patient’s Snore Score, based on the average volume and duration of snoring, decreased from 50 at baseline to 30 after 1 month, 19 after 2 months, 10 after 3 months, and 2-4 after 4 months. After 1 year of combined aligner and ASA treatment, a follow-up sleep study was performed by the patient’s sleep physician. As shown in Table 1, multiple measures of OSA severity were improved by the treatment, including the number of apneas, hypopneas, and respiratory effort-related arousals, as well as oxygen saturation. The patient underwent a repeated sleep study with both the Aligner Sleep Appliance (ASA) and clear aligners in place. Upon the completion of active aligner therapy at 14 months, the patient had his teeth restored with Zirconia veneers – from #5 to #12 and from #22 to #27 (Figures 11-13).

After the patient completed their orthodontic and restorative treatment, the retention of the ASA with clear aligners was not optimal. We presented two treatment options: the first was to proceed with the ASA and clear aligners as they were, and the second was to use a new appliance, the Respire Blue, which had better retention and could be worn without the clear aligners. He planned to wear his clear aligner retainers for 2 hours during the day, and ordered a Respire Blue oral appliance (Whole You Dental Laboratory, Brooklyn, USA) with the same settings as the ASA for night wear. The patient was placed on a recall schedule according to standards of the American Academy of Dental Sleep Medicine (every 6 months for the first year and once a year after). 7 He was advised to see his sleep doctor every year for sleep evaluation.
Discussion
The case presented here is a notable example of a complex patient presentation requiring a multi-disciplinary approach. Our patient needed simultaneous treatment for OSA and a dental malocclusion. Clear aligners were paired with a new generation oral appliance, the ASA, to simultaneously correct the malocclusion and alleviate pre-existing OSA. As a result, the patient’s OSA significantly improved (see Table 1) with both the apnea-hypopnea index (AHI) and supine AHI decreasing from moderate/severe levels to clinically minimal. Our hope is that this report will help guide other practitioners in how dental interventions can be customized and combined with myofunctional therapy and nasal irrigation to treat patients with complex dental sleep conditions.
Combining oral appliance therapy with orthodontic and restorative treatment can be a controversial approach, but an Aligner Sleep Appliance in combination with clear aligners can address the misalignment of the teeth, achieve restorative goals, and provide a solution for OSA patients who have crowded, misaligned teeth that impinge on tongue space and force the tongue into the airway. The use of the ASA with modified clear aligners during restorative treatment can be an effective approach.
It also has the potential to offer a useful solution for practitioners who are preparing their patients for orthognathic surgery to correct OSA. Most patients who seek orthognathic surgery have misaligned teeth and have not been able to tolerate CPAP therapy.
Conclusion
In the future, when you encounter a patient with OSA who is also interested in straightening their teeth, you don’t have to inform them that using CPAP is the only way to maintain proper breathing during clear aligner treatment.
Some patients who can’t tolerate CPAP can try the Aligner Sleep Appliance (ASA). Read about the many options for OSA patients in this continuing education article, “Precision Medicine in a Dental Sleep Practice,” that discusses efficient clinical workflow and patient selection for various treatments at https://dentalsleeppractice.com/ce-articles/precision-medicine-dental-sleep-practice/. Subscribers can take the quiz and obtain 2 CE credits!
 As a founder and CEO of Harmony Dental Arts, Dr. Maria Sokolina is very passionate about making the world a more beautiful and more healthy place with sound sleep and healthful breathing. Dr. Sokolina emigrated from Russia with her first medical degree, and later received her DDS degree from New York University College of Dentistry. Upon graduation, Dr. Sokolina pursued specialized skills in different areas of dentistry such as implants, cosmetic dentistry, full mouth rehabilitation, and orthodontics. As part of her practice, Dr. Sokolina became an active explorer of the world of Dental Sleep Medicine, trying to find a cure for sleep apnea with dental appliances and myofunctional therapy. Dr. Sokolina is a lecturer and Diplomat of American Academy of Dental Sleep Medicine. Dr. Sokolina is a Board member of the American Academy of Dental Sleep Medicine as well as TEDx. Dr. Sokolina spends much of her professional time trying to spread knowledge with lectures about “Sleep, Breath and Wellness” among the general population as well as in the medical community. She may be contacted through her website at https://www.harmonydentalarts.com/.
As a founder and CEO of Harmony Dental Arts, Dr. Maria Sokolina is very passionate about making the world a more beautiful and more healthy place with sound sleep and healthful breathing. Dr. Sokolina emigrated from Russia with her first medical degree, and later received her DDS degree from New York University College of Dentistry. Upon graduation, Dr. Sokolina pursued specialized skills in different areas of dentistry such as implants, cosmetic dentistry, full mouth rehabilitation, and orthodontics. As part of her practice, Dr. Sokolina became an active explorer of the world of Dental Sleep Medicine, trying to find a cure for sleep apnea with dental appliances and myofunctional therapy. Dr. Sokolina is a lecturer and Diplomat of American Academy of Dental Sleep Medicine. Dr. Sokolina is a Board member of the American Academy of Dental Sleep Medicine as well as TEDx. Dr. Sokolina spends much of her professional time trying to spread knowledge with lectures about “Sleep, Breath and Wellness” among the general population as well as in the medical community. She may be contacted through her website at https://www.harmonydentalarts.com/.
Disclaimer: Dr. Sokolina has no financial involvement with SleepArchitx nor with Invisalign.
- Kandasamy S, Goonewardene M. Class II malocclusion and sleep-disordered breathing. Seminars in Orthodontics. 2014;20(4):316-323. doi:10.1053/j.sodo.2014.09.007
- Balasubramaniam R, Klasser GD, Cistulli PA, Lavigne GJ. The link between sleep bruxism, sleep disordered breathing and temporomandibular disorders: an evidence-based review. J Dent Sleep Med. 2014;1(1):27–37.
- Bonsignore MR, Baiamonte P, Mazzuca E, Castrogiovanni A, Marrone O. Obstructive sleep apnea and comorbidities: a dangerous liaison. Multidiscip Respir Med. 2019;14(1):8. doi:10.1186/s40248-019-0172-9
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The Occurrence of Sleep-Disordered Breathing among Middle-Aged Adults. N Engl J Med. 1993;328(17):1230-1235. doi:10.1056/NEJM199304293281704
- Weaver TE, Grunstein RR. Adherence to Continuous Positive Airway Pressure Therapy: The Challenge to Effective Treatment. Proceedings of the American Thoracic Society. 2008;5(2):173-178. doi:10.1513/pats.200708-119MG
- Ataii, Payam. Performing Orthodontics While Treating OSA. Inside Dentistry. 2019;15(2). Accessed April 21, 2022. https://www.aegisdentalnetwork.com/id/2019/02/performing-orthodontics-while-treating-osa
- Ramar K, Dort LC, Katz SG, et al. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015: An American Academy of Sleep Medicine and American Academy of Dental Sleep Medicine Clinical Practice Guideline. Journal of Clinical Sleep Medicine. 2015;11(07):773-827. doi:10.5664/jcsm.4858