by Earl O. Bergersen, DDS, MSD
 Sleep-Disordered Breathing in Children can manifest itself in various symptoms that can easily be overlooked, misdiagnosed, and be left untreated. Common labels placed on these children are ADD/ADHD. It is extremely important for the dental community to understand sleep-disordered breathing, the cause, the cure, and how to treat.
Sleep-Disordered Breathing in Children can manifest itself in various symptoms that can easily be overlooked, misdiagnosed, and be left untreated. Common labels placed on these children are ADD/ADHD. It is extremely important for the dental community to understand sleep-disordered breathing, the cause, the cure, and how to treat.
Sleep-disordered breathing occurs when there is interference of the free passage of air to and from the lungs through the nose and pharynx often called sleep disordered breathing; hypopnea (low breathing) and apnea (complete stoppage) which interrupts a child’s sleep cycle and prevents them from completing a full night’s sleep and often has serious medical implications. Both of these symptoms can be present from birth to any age. Nighttime mouth breathing also occurs frequently in children. Any child that snores fairly frequently and sleeps with their mouth open often suffers from lack of sleep and as a result also frequently has oxygen desaturation of the blood. The various symptoms listed below occur in about 1 out of 5 children who often snore.
Early intervention is effective in the deciduous through transitional dentition (4 to 10 years of age) to successfully treat children with sleep problems. There are several serious symptoms that can occur in children with improper sleep habits:
- Snoringfrom2to7nightsperweek
- Hyperactivity
- Excessivedaytimesleepiness
- Daytimeand/ornighttimemouthbreathing
- Attentiondeficit
- Toothgrinding
- Restless sleep
- Throatinfections
- Difficultbreathingwhilesleeping
- Bedwetting
- Poorabilitytostudy
- Headachesinthemorning
- Sleeptalking
- FallingasleepwatchingTV
- Allergicsymptoms
- Awakeningatnight
These common symptoms are over 2 times more prevalent in habitual snorers (5 to 7 nights per week) than in non-snorers (16.8% vs. 40.2%). In fact, in those children that snore periodically (2 to 4 nights per week) have 1.6 times the incidence of these 16 symptoms over those children that do not snore (16.8% vs 26.1%).1,2
How to Identify, Treat, And Cure
A dentist is often the first in line to diagnose abnormal breathing symptoms, and is the logical person to initiate treatment of any associated orthodontic problems. As a result, the dentist can also be the one to initiate such interceptive treatment that can greatly benefit the young patient.
The Perfect Start Treatment is designed to address interrupted breathing habits. Sleep deprivation in children, particularly between 3 and 10 years of age, most often affects their behavior and these characteristics are often strong indications of problems
A Dentist should get more information from the parent by having them fill out a questionnaire.
Several important questions should be asked of the parent of a young child of 3 to 10 years of age. The following questions are the important ones to ask a parent:
- Does your child snore?
- Does the snoring occur 2 to 4 nights a week (moderate snoring)?
- Or does it occur 5 to 7 nights a week (habitual snoring)?
- Is it interrupted snoring where the child stops breathing?
- Does this interrupted snoring last 4 seconds or more at least twice per hour?
- Is your child hyperactive?
- Does your child lack attention (attention deficit)?
- Does the child have headaches in the morning?
- Sweat profusely while sleeping?
- Is your child fidgety?
- Do you have trouble understanding the child’s speech?
- Have trouble pronouncing consonants like P, B, V, T, etc.
- Is the child a restless sleeper?
- Look sleepy during the day?
- Does poorly in school, particularly in mathematics or spelling?
- Does your child breathe through
the mouth? - Does your child often wet the bed at night?
- Does your child grind his or her teeth?
- Does your child often have nightmares?
(Sahim et al, 2009; Urschitz et al, 2004)
Reviewing data (from Sahin, Eitner, and Guenther, 2004) indicate that ADD, ADHD, daytime sleepiness, restless sleep, daytime mouth breathing, bed wetting, tooth grinding, poor school performance and morning headaches are 290% more prevalent in the habitual snorers than in non-snorers. Swollen tonsils and adenoids should be routinely checked on all children.
Testing for poor sleep breathing for children is done with polysomnography — the overnight sleep study; if apneic events and lowered blood oxygen are found, physicians most often prescribe surgery or PAP therapy. Typical dental appliances that advance the mandible in adults are not appropriate for treating airway issues in children, since they may cause excessive lower jaw growth. It takes a growth-oriented approach for dentists to impact airway health.
Treatment
The Perfect Start System is a series of specially designed appliances that are provided to help promote proper breathing habits. The system addresses mouth breathing, an open-bite, narrow palate, sucking and swallowing problems, and speech difficulties. The system prevents the mandible from slipping posteriorly while sleeping which stops the snoring, maintains an open airway, and can prevent many of the symptoms of sleep-disordered breathing.
 The advancement of the mandible can stimulate 54% more mandibular growth when compared to a similar control sample from 5 to 8 years of age.3,4 The Perfect Start™ treatment moves the lower jaw in an anterior direction in the proper amount while also advancing the tongue. The Perfect Start System has the effect of increasing the pharyngeal space between the base of the tongue and the posterior wall of the pharyngeal airway.
The advancement of the mandible can stimulate 54% more mandibular growth when compared to a similar control sample from 5 to 8 years of age.3,4 The Perfect Start™ treatment moves the lower jaw in an anterior direction in the proper amount while also advancing the tongue. The Perfect Start System has the effect of increasing the pharyngeal space between the base of the tongue and the posterior wall of the pharyngeal airway.
The Perfect Start™ System treats additional orthodontic problems such as crowding, overbite, overjet, gummy smiles and lack of coordination between the arches. These conditions can be corrected with the Perfect Start™ System will little or no future relapse of the correction.
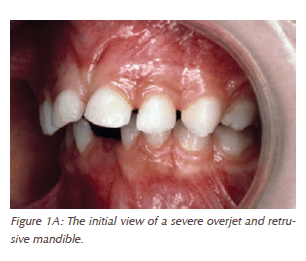
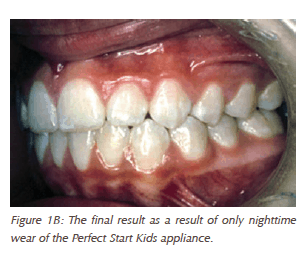 A typical example of the mandibular advancement possible with the Perfect Start Kids™ appliance is seen in Figures 1A-1B. One should always be aware that children with recessive mandibles are also strong candidates for restricted pharyngeal airways and sleep-disordered breathing.
A typical example of the mandibular advancement possible with the Perfect Start Kids™ appliance is seen in Figures 1A-1B. One should always be aware that children with recessive mandibles are also strong candidates for restricted pharyngeal airways and sleep-disordered breathing.
For further information on The Perfect Start™ System, please visit www.perfectstart.com, e-mail info@perfectstart.com, or call 1-844-413-2166.
References
1. Sahin U, Ozturk O, Ozturk M, Songur N, Bircan A, Akkaya A. Habitual Snoring in Primary School Children: Prevalence and Association with Sleep-Related Disorders and School Performance. Med Princ Pract. 2009; 18:458-465. 2. Urschitz MS, Eitner S, Guenther A, et al. Habitual Snoring, Intermittent Hypoxia, and Impaired Behavior in Primary School Children. Pediatrics. 2004; 114:1041-1048. 3. Keski-Nisula, K., Keski-Nisula, L., Salo, H., Volpio, K., and Varrela, J., Dentofacial changes after orthodontic intervention with Eruption Guidance Appliance in the early mixed dentition. Angle Orthod., 78: 324-331, 2008. 4. Katri Keski-Nisula, DDS, Raija Lehto, DDS, Vuokko Lusa, DDS, Leo Keski-Nisula, MD, PhD, and Juha Varrella, DDS, PhD, Occurance of malocclusion and need of orthodontic treatment in early mixed dentition. AJO-DO, vol. 124, no. 6, 2003.