As the final article in the 4-part series, Sharon Moore shows how dental practices can offer sleep education, screening, and treatment for many breathing challenges related to children’s sleep-disordered breathing.
 by Sharon Moore
by Sharon Moore
In the final installment of this four-part series, author, speech pathologist, and myofunctional practitioner Sharon Moore shares critical information about sleep disordered breathing, an under-recognized disorder taking a toll on children’s health, development and quality of life.1 When children’s sleep and breathing improve, they are happy, alert and better behaved within days, and having a healthy airway from a young age can save kids (and parents) from a lot of trouble later in life.
Sleep is a global health challenge, which is why we should screen every child for sleep health and sleep disordered breathing (SDB) specifically. By doing so in my clinic, we frequently encounter families whose children have disrupted sleep, wake frequently or consistently, have signs of insomnia, wake unrefreshed, have nightmares, wet the bed and more.
Yet many parents say, in the face of these reported sleep behaviors, they think their child is getting good sleep, despite accompanying daytime ‘shenanigans.’2 They feel confident that if their child spends the right number of hours in bed, their sleep must be sufficient. Meanwhile, others acknowledge worrying sleep and daytime behaviors but dismiss these as part of the norm when raising kids.
Why is this? Sleep myths and misperceptions persist among the public, my dental colleagues, and medical professionals. This interferes with sleep health being taken seriously, leading many to believe that poor sleep is to be endured in the trenches of parenting.
It does not need to be this way. Any signs of sub-optimal sleep beg the big question – Why?
When it comes to breathing during sleep, in the absence of obstructive sleep apnea (OSA), other breathing challenges along the spectrum of SDB may be responsible.3-5
The Spectrum of SDB
SDB is a broad term for breathing difficulties occurring during sleep. Consequently, there is a range of disorders on the spectrum, including, OSA, snoring, upper airway resistance syndrome (UARS), respiratory effort related arousal (RERA) and even mouth breathing.
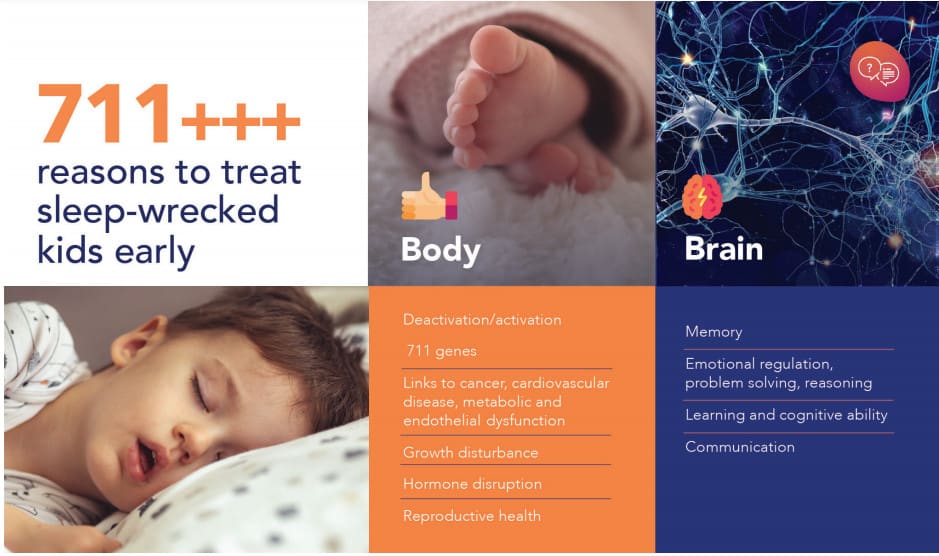
While snoring and mouth breathing often aren’t seen as serious issues by parents and professionals, the truth is that any breathing difficulties will lead to disruption of the sleep architecture that is fundamental to the brain cleansing and restoration (glymphatics) that must happen every single night for the brain to fully restore and regenerate to be ready for the next day.6 This then leads to a range of developmental and behavioral consequences.
Knowing that sleep-disordered breathing is on a continuum, and that problems do not cease simply because of a numerical measurement like the Apnea Hypopnea Index (AHI), raises questions about how to recognize and treat upper airway issues that are deemed ‘less severe’ on the SDB continuum, or indeed not recognized at all.
The Importance of Screening for SDB
Currently, validated pediatric sleep questionnaires are designed to identify OSA. This is very important because OSA is a life-threatening disorder with serious consequences. However, what happens when kids don’t have OSA but they still have a problem like UARS?
That’s why I use a signs and symptoms questionnaire as it adds to the clinical picture and also provides a mechanism to discuss sleep and breathing with parents, including what’s normal and what’s not. The clinical questions raised include: What if there is airway narrowing, collapse or obstruction at some point in the airway that makes breathing laborious? What if there is fast or noisy breathing, raising body temperature and heart rate, but not actually lowering oxygen?
Breathing issues activate the sympathetic nervous system, disrupt sleep architecture, fragment sleep, and may be the reason why kids wake at night.7 Kids with these problems can suffer the same daytime physical, mental, emotional, and social consequences as a child with OSA, but they may be misdiagnosed as having anxiety or ADHD, oppositional defiance, depression, autism, PTSD, aggression, emotional fragility, or learning problems. They may wet the bed or have unexplained waking and the wrong treatment may be prescribed. If the problem is due to SDB, no amount of psychological support, bells, whistles, or pharmaceuticals will fix this problem. Fixing the airway and breathing will.8
This illustrates an important point: Generally, insomnia is placed into the basket of stress and emotional issues. However, Dr Barry Krakow’s work on complex insomnia clearly demonstrates the underlying reason for waking can be related to breathing events that rouse a person out of the normal sleep phase and stage, activating the sympathetic nervous system, elevating heart rate and blood pressure. Dr. Krakow found that 90% of awakenings experienced by insomniacs were preceded by a disruption in their breathing while asleep, demonstrating a physiological breathing problem in thousands of insomnia patients over two and a half decades.9-12
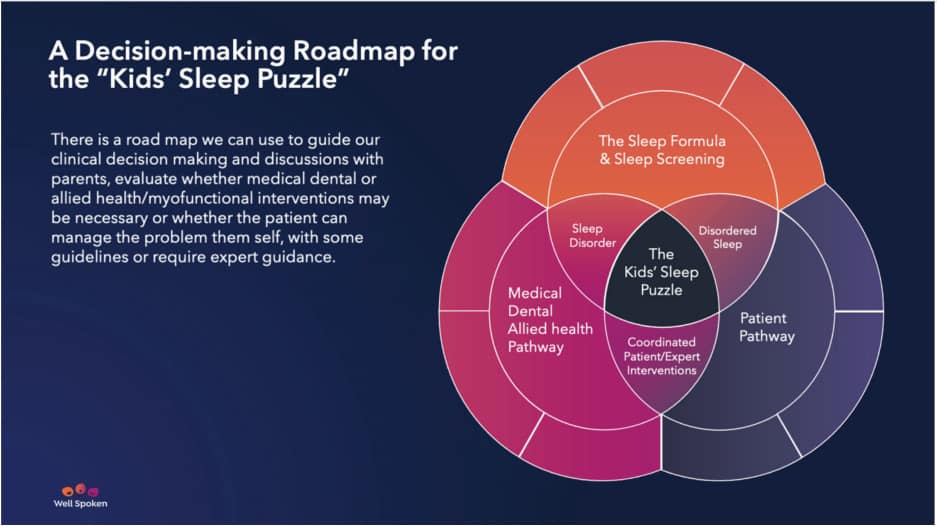
The Kids’ Sleep Puzzle
There is a roadmap we can use to guide our clinical decision making and discussions with parents, including evaluating whether medical, dental or allied health or myofunctional interventions may be necessary. Here is a framework to guide decision making about the next steps:
The Sleep Formula & Sleep Screening
Simply start: Screen every child for
- sleep problems
- SDB
- triage symptoms for treatment urgency
The Patient Pathway
Provide patient education to improve, sleep health practices, optimizing environment, behavior & routines, and tips for upper-airway health like keeping the nose clear, managing allergies, middle ear effusion, food intolerances or reflux. Furthermore, being ‘airway fit’ is critical i.e. ensuring the muscles systems that support healthy airway are optimized. Myofunctional therapy is an important feature of upper airway health and function.
…a child with OSA…may be misdiagnosed as having anxiety or ADHD, oppositional defiance, depression, autism, PTSD, aggression, emotional fragility, or learning problems.
Medical, Dental, and Allied Health Treatment Pathway
The American Dental Association’s 2017 Policy Statement on the Role of the Dentist in Sleep Disordered Breathing specifies that recognition of SDB is now a part of the dental profession and recommends that every dental practice screen for SDB, even if patients are subsequently referred for treatment elsewhere.13,14
If a patient requires expert medical, dental, or allied health assessment & treatment, decide:
- When: Triage the urgency
- Who: Decide who needs to be involved and make referral(s)
- What: And if your dental practice is a treatment provider, a detailed ‘airway’ structural and functional assessment and treatment plan can be activated.
Dental practices can offer sleep education, screening, and treatment with the aim of treatment as early as possible. Remember, myofunctional interventions sit alongside dental treatments until upper airway muscle functions are ‘normalized or ‘optimized’. Being on the frontline, dentists are in the best position to encourage the whole family to think about sleep health. We have a window of opportunity to guide families so that every child gets the sleep they need every night (and parents, too)!
It has been such a pleasure write these four articles dedicated to pediatric sleep with a dental and myofunctional focus. Time and time again, we see the essential role of dentists in screening, education and treatment of SDB. If you would like to learn more about sleep issues in kids and how to address them, please read my book Sleep Wrecked Kids and look out for part 1, 2, & 3 of a new publication coming: Well Slept Kids: A step-by-step guide to transforming your child’s sleep before they start school. For queries: email projects@wellspoken.com.au or visit http://www.wellspoken.com.au.
Sharon Moore shows how adult and children’s sleep-disordered breathing can affect the mental, emotional, and physical wellbeing of patients of any age. Read about the link between sleep and airway in “The Future Face of Sleep” here: https://dentalsleeppractice.com/the-future-face-of-sleep/
 Sharon Moore is an author, speech pathologist and myofunctional practitioner with 40 years of clinical experience across a range of communication and swallowing disorders. Sharon has a special interest in early identification of craniofacial growth anomalies in children, concomitant orofacial dysfunctions, and airway obstruction in sleep disorders.
Sharon Moore is an author, speech pathologist and myofunctional practitioner with 40 years of clinical experience across a range of communication and swallowing disorders. Sharon has a special interest in early identification of craniofacial growth anomalies in children, concomitant orofacial dysfunctions, and airway obstruction in sleep disorders.
- Sharon Moore, Sleep-Wrecked Kids: Helping Parents raise happy healthy kids one sleep at a time. (New York: Morgan James publishing, November 2019).
- Sharon Moore, Sleep-Wrecked Kids: Helping Parents raise happy healthy kids one sleep at a time. (New York: Morgan James publishing, November 2019).
- Guilleminault C., Stoohs R., Clerk A., Cetel M., Maistros P.A cause of excessive daytime sleepiness: the upper airway resistance syndrome. Chest1041993781787
- Arnold WC, Guilleminault C. Upper airway resistance syndrome 2018: non-hypoxic sleep-disordered breathing. Expert Rev Respir Med. 2019 Apr;13(4):317-326. doi: 10.1080/17476348.2019.1575731. Epub 2019 Feb 6. PMID: 30689957.
- Guilleminault C., Black J. E., Palombini L., Ohayon M.A clinical investigation of obstructive sleep apnea syndrome and upper airway resistance syndrome patients. Sleep Med 1200016
- Plog BA, Nedergaard M. The Glymphatic System in Central Nervous System Health and Disease: Past, Present, and Future. Annu Rev Pathol. 2018;13:379-394. doi:10.1146/annurev-pathol-051217-111018
- Lopes MC, Spruyt K, Azevedo-Soster L, Rosa A, Guilleminault C. Reduction in Parasympathetic Tone During Sleep in Children With Habitual Snoring. Front Neurosci. 2019 Jan 10;12:997. doi: 10.3389/fnins.2018.00997. PMID: 30686970; PMCID: PMC6335331.
- Di Carlo, G.; Zara, F.; Rocchetti, M.; Venturini, A.; Ortiz-Ruiz, A.J.; Luzzi, V.; Cattaneo, P.M.; Polimeni, A.; Vozza, I. Prevalence of Sleep-Disordered Breathing in Children Referring for First Dental Examination. A Multicenter Cross-Sectional Study Using Pediatric Sleep Questionnaire. J. Environ. Res. Public Health2020, 17, 8460.
- Krakow B, McIver ND, Ulibarri VA, Nadorff MR. Prospective Randomized Controlled Trial on the Efficacy of Continuous Positive Airway Pressure and Adaptive Servo-Ventilation in the Treatment of Chronic Complex Insomnia, The Lancet, EClinicalMedicine 13 (2019) 57–73
- Krakow B, McIver ND, Ulibarri VA, Nadorff MR. Retrospective, nonrandomized con- trolled study on autoadjusting, dual-pressure positive airway pressure therapy for a consecutive series of complex insomnia disorder patients. Nat Sci Sleep 2017;9: 81–95.
- Krakow B, Melendrez D, Sisley B, Warner TD, Krakow J, Leahigh L, et al. Nasal dilator strip therapy for chronic sleep-maintenance insomnia and symptoms of sleep- disordered breathing: a randomized controlled trial. Sleep Breath 2006;10(1): 16–28 March.
- Krakow B, McIver ND, Ulibarri VA, Nadorff MR. Frequency and accuracy of “RERA” and “RDI” terms in the journal of clinical sleep medicine from 2006 through 2012. J Clin Sleep Med. 2014; 10: 121-124
- ADA Policy Statement: The Role of Dentistry in the Treatment of Sleep Related Breathing Disorders.Adopt ed 2017
- American Association of Orthodontists. (2019). Obstructive sleep apnea and orthodontics [White Paper]. https://www1.aaoinfo.org/wp-content/uploads/2019/03/sleep-apnea-white-paper-amended-March-2019.pdf. Accessed June 21, 2019.