
Laura Sheppard writes about selecting oral appliances and consideration for achieving the best fit for effective retention.
by Laura Sheppard, BS, CDT, TE
You Are Not Your Patient – Expand Your Toolbox
Many practitioners make it a standard procedure to try out all types of devices on themselves, so they can assess fit, comfort, ease of insertion, removal, and adjustment. This is commendable. However, it can also be a slippery slope. Your patient is not you. I often hear doctors say they did not like one aspect or another of a device when they tried it, so they would not recommend it for their patients. This often leads to prescribing only one or two types of appliances to serve their patients’ needs. This may be a mistake. For best results, select an appliance based on the consult considerations listed below.
If you are using the wrong tools or if you are using the correct tools in the wrong way, the results are the same.
So Many Choices
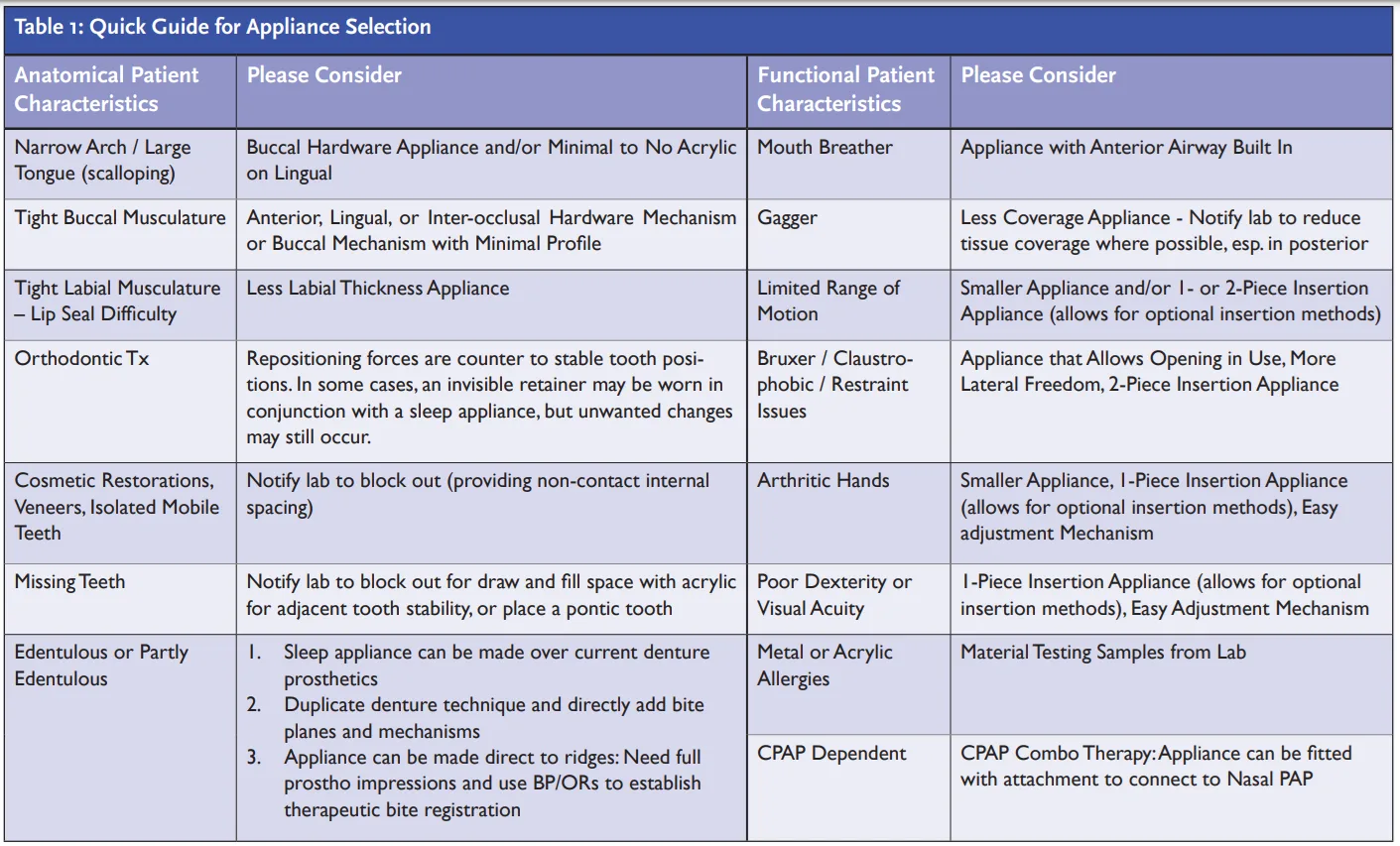
Appliance selection requires an understanding of the appliance designs AND a careful analysis of your patient to select the best option. If in doubt, contact your lab for some insight. Lab consultations are especially helpful when you are not sure which appliance is best. A lab discussion should include the patient’s dental condition, stability, bruxer or clencher, missing teeth or any extreme dental contours. Is the patient an oral or nasal breather? What is the amount of tongue space (tongue scalloping, tongue biter) and character of facial musculature (cheek biter, tight or loose facial musculature, difficulty getting a lip seal, etc.)? Are they currently or formerly a sleep appliance wearer? Or are they currently or recently an orthodontic patient?
With this information, your lab should be able to help you understand the common pitfalls and determine the best type of appliance for your patient. (See Table 1 for a quick guide for appliance selection.)

Retention Challenges
The Quad Challenge x 4! The most critical element of any oral appliance is fit and retention. Let’s just start by looking at a single arch device. As you know, depending on the dental anatomy, any type of single-arch, full-coverage appliance like a splint or a retainer can be challenging to passively insert, remove, fit comfortably and be retentive. This is known as the ‘quad challenge’. Now, let’s take an oral sleep appliance involving both arches. With a sleep appliance this singular-arch quad challenge has just multiplied its complications by yet another 4 challenges!
- Obtaining fit, retention and comfort on two arches.
- Facilitating insertion, connection, and removal as 2 pieces (or in some cases, 1 piece) while being influenced by the arc of closure in protrusive.
- Insuring U/L retention during wear & stress, factoring in the confinement of muscular movements and the constant downward forces of the mandible (if U/L appliances are connected).
- Managing the voluntary or involuntary expression of muscular actions during sleep, causing dislodgement and/or fractures.

Too much retention is infinitely more common in natural dentition than cases lacking it. The cases where teeth are very curvaceous, triangular, tipped or crowded, missing, or perio-involved with root exposure require careful survey of the path of insertion, blocking out of severe undercuts in advance of manufacture, or relieving the appliance material during seating. Of course, the risk lies in removing too much undercut and rendering a loose fit. Labs today can survey the case with scan & digital design technology, or they can use a manual surveyor.
Not enough retention presents even more challenges. How to create retention where none exists? On cases with short crowns or minimal height of contour, it may be necessary to have buccal undercuts added. Usually, 4 points of retention on the arch is sufficient. Points of retention are commonly placed at the first bicuspids and first molars. You can do this free-hand by building up composite ledges to replicate buccal bulges at the mid-cervical of the teeth.
Another option is to bond a pre-form wedge like the wedges used with invisible aligners. Note: Figure 1 shows wedges placed for alignment. To use this concept for retention, the locking ledge is placed cervically on posteriors to allow for the appliance to snap over. You may decide to soften the severity of the edges based on trial fitting.
My preferred product has always been bondable Crown Contour Attachments from TruTain (Figure 2). These are clear, pre-formed buccal bulges that you can bond in place via light cure. They have a small handle on them that once bonded in place can be twisted off and discarded. Super easy and fast.
When selecting oral appliances, your office should have a compliance plan. Read “Provision of Oral Appliances and Regulatory Compliance: Why Your Practice Should Have a Compliance Plan” by Jayme R. Matchinski, Esq. to find out more about demonstrating regulatory compliance in the event of an audit, investigation, or other enforcement activity. https://dentalsleeppractice.com/provision-of-oral-appliances-and-regulatory-compliance-why-your-practice-should-have-a-compliance-plan/
 Laura Sheppard BS, CDT, TE, is a practicing 40 year board-certified dental laboratory technician with her AAS in Dental Technology and BS in Education for Allied Health. Named to the ‘Top 25 Women in Dentistry’ roster by Dental Products Report, Laura has been nationally recognized and published as an expert and educator in the development and implementation of Dental Sleep Medicine and Quality Systems since 1993. As the design collaborator for DSG APM Positioner™ and DSG Remed-eze™, inventor for DSG Relaxer™, and co-inventor of MicrO2™ aka ProSomnus® AI, Laura’s expertise and contributions in dental sleep device invention, design, manufacturing, and regulatory compliance has been utilized to the success of many of today’s advanced sleep devices.
Laura Sheppard BS, CDT, TE, is a practicing 40 year board-certified dental laboratory technician with her AAS in Dental Technology and BS in Education for Allied Health. Named to the ‘Top 25 Women in Dentistry’ roster by Dental Products Report, Laura has been nationally recognized and published as an expert and educator in the development and implementation of Dental Sleep Medicine and Quality Systems since 1993. As the design collaborator for DSG APM Positioner™ and DSG Remed-eze™, inventor for DSG Relaxer™, and co-inventor of MicrO2™ aka ProSomnus® AI, Laura’s expertise and contributions in dental sleep device invention, design, manufacturing, and regulatory compliance has been utilized to the success of many of today’s advanced sleep devices.