CE Expiration Date: April 15, 2028
CEU (Continuing Education Unit):2 Credit(s)
AGD Code: 730
Educational Aims
This self-instructional course for dentists suggests various ways to think about Sleep Related Breathing Disorders (SRBD) and pre-disease as it relates to children with malocclusion. The article describes how clinicians must give systematic attention to creating collaborative environments in which dentists, otolaryngologists, and sleep medicine practitioners can work in concert to screen, evaluate, and treat childhood SRBD within the parameters of evidence-based medicine.
Expected Outcomes
Dental Sleep Practice subscribers can answer the CE questions online to earn 2 hours of CE from reading the article. Correctly answering the questions will demonstrate the reader can:
- Realize the historical context behind the diagnosis and treatment of SRDB-Malocclusion in the pre-WW II era, prior to the era of evidence-based medicine.
- Realize the impact of the ADA House of Delegates 2017 policy statement on the role of dentists in screening and treating SRBD and referring affected patients to appropriate physicians.
- Identify several SRBD screening tools currently being utilized for assessment of pediatric sleep hygiene status.
In this CE, Dr. Kevin Boyd talks about creating collaborative environments for diagnosing and treating young patients with malocclusion and SRBD. Subscribers can take the CE quiz and receive 2 CE credits!
 What Needs to Be Done Now Has Been Done Before
What Needs to Be Done Now Has Been Done Before
by Kevin Boyd, DDS, MSc
To best help their patients, dentists and other allied health professionals like to consider their continuing education endeavors as being current, fresh, and challenging, with novel ideas. There should be strong evidence to back up a change in how they evaluate and plan both preventive and active therapy. Much of today’s norms of medical care were set decades before randomized control trials (RCT’s) became the standard after WW II. In the absence of robust data derived from RCT’s, dentists can seek out from peer-reviewed literature the best available evidence to identify children who might be deemed at-risk of disease. Further evaluation and treatment, when their present and future health might become compromised by waiting, is prevention in action. When suffering is obvious, children might need more complex and possibly critical care. This essay will show the wisdom of clinicians from decades ago and discuss screening tools. It suggests ideas to bring patients and collaborating colleagues into new and effective ways to think about disease and pre-disease.
Pediatric Respiratory Hygiene: Historical Context of a Modern Medical-dental Dilemma
At the1921 annual meeting of the American Academy of Dental Science, distinguished Boston orthodontist Dr. Leroy Johnson presented, ‘The Diagnosis of Malocclusion with Reference to Early Treatment’. Dr. Johnson confidently concluded, ‘The face has evolved with the functions of mastication and respiration. The perversion of either or both functions will result in some degree of modification of the structure of the jaws. This the law of biology….’.1 Similar observations had been expressed at a New York medical meeting in 1912 by physician-dentist EA Bogue: 2 “When the dental arch is narrow, the nasal openings are also narrow, and are accompanied with more or less nasal stenosis…..A large percent of these cases are caused by the lack of natural capacity, due largely to the contracted dental arch and nares…..The roof of the mouth is the floor of the nose…The proper lateral expansion of the upper dental arch especially in young patients, while in their developmental stage increases the narial openings and improves the breathing capacity….”
Where’s the Evidence?
As these two particular early 20th-Century scientific meetings had preceded the era of evidence-based medicine (EBM) by several decades,3 Drs. Johnson and Bogues’ statements could not have been based upon conclusions gleaned from carefully constructed random control trial (RCT) designed studies. Dentists today should seek to be guided by the best available evidence.4 Consider, however, that neither Dr. John Snow’s conclusions about the casual relationship between consumption of water from a contaminated community well and the contagiousness of cholera,5 nor Dr. Ignaz Semmelweis’ conclusion about the importance of physicians washing their hands after necropsy dissection prior to delivering babies6 had been based upon RCT-derived data. Within the context of informing best clinical practices when/where RCT-derived data might be unavailable, not possible or impractical to obtain per IRB ethical constraints or financial resource restrictions, the usefulness of research data that are sometimes derived from observational study design is well established in the scientific literature.7
A commonly held position is that controlled trials of an observational vs. randomized trial design can be useful towards generating accurate and clinically useful data where and when RCT’s cannot or have failed to do so. In support of this idea, the editors of JAMA-Pediatrics recently published data from a well-designed observational trial regarding potential fetal neurotoxicity of maternal fluoride intake as measured from the mothers’ urinary excretion.8 To publish data from this non-RCT was an unusual policy decision according to JAMA editors. In addition, the data were so compelling that JAMA issued a recommendation regarding excessive maternal fluoride intake.
Dx: SRDB-Malocclusion Co-morbidity: Pre-WW II Physician-Dentist Collaboration
There are numerous pre-WW II papers published within the corpus of medical and dental literature that support the practice of physicians and dentists collaboratively diagnosing and treating SDB and malocclusion co-morbidity, mostly skeletal-dental maxillary transverse deficiency and mandibular distal occlusion (retrusion/retrognathia) through the ‘spreading of the deciduous arches’ during the early childhood years (30 months-7 y.o./complete primary-early mixed dentitions).2,8 These interventions had been carried out for the primary purpose of improving nasal breathing and quality of life rather than solely for the purpose of correcting so-called ‘irregularities of the teeth’. As these historically important journal articles pre-dated the 1948 initial published report of an RCT by several decades, it is unreasonable to criticize their usefulness compared to current RCT standards. Developing malocclusions are nearly always first detectable in the primary dentition (ages 2.5-7 yrs),9,10 nearly always become more complex (i.e., get worse) with age without appropriate intervention,9 and are very frequently co-morbid with pediatric sleep related breathing disorders (SRBD). In the single-digit growth years they are non-surgically correctible with validated orthodontic/dentofacial orthopedic interventions. It seems reasonable to suggest that failure to diagnose and appropriately treat or refer afflicted young children is a medically-indefensible position.
Recent Events
In 2017, the ADA House of Delegates approved a policy statement on the role of dentists in treating SRBD.11 Key components include assessing a patient’s risk for SRBD as part of a comprehensive medical and dental history and referring affected patients to appropriate physicians. Specifically, the policy statement refers to the screening of children:
In children, screening through history and clinical examination may identify signs and symptoms of deficient growth and development, or other risk factors that may lead to airway issues. If risk for SRBD is determined, intervention through medical/dental referral or evidenced based treatment may be appropriate to help treat the SRBD and/or develop an optimal physiologic airway and breathing pattern.
It is widely believed that current dental education does not prepare dentists to recognize pediatric airway issues. Standardized methods of screening with recognized thresholds for referral are not currently available. Development of these metrics would displace the subjective criteria that are currently used and provide a common language for every provider on the child’s health care team. Contemporaneous educational materials on the screening methods and the significant signs of pediatric airway issues would benefit the dental community and public.
Pediatric SRBD Screening: Birth History Factors, Behavioral and Physical Traits
SRBD-PSQ Behavioral Scale
Several SRBD screening tools are currently being utilized for assessment of pediatric sleep hygiene status. Two commonly used tools are B.E.A.R.S.12 and Dr. Ron Chervin’s Pediatric Sleep Questionnaire (PSQ),13 a 22-question SRBD scale that has strong correlation with overnight polysomnography sleep test (PSG) metrics for determining a child’s sleep quality. The PSQ can be highly predictive of increased risk for SRBD neurobehavioral morbidity and risk of post-adenotonsillectomy OSA recurrence as well as or better than PSG.14
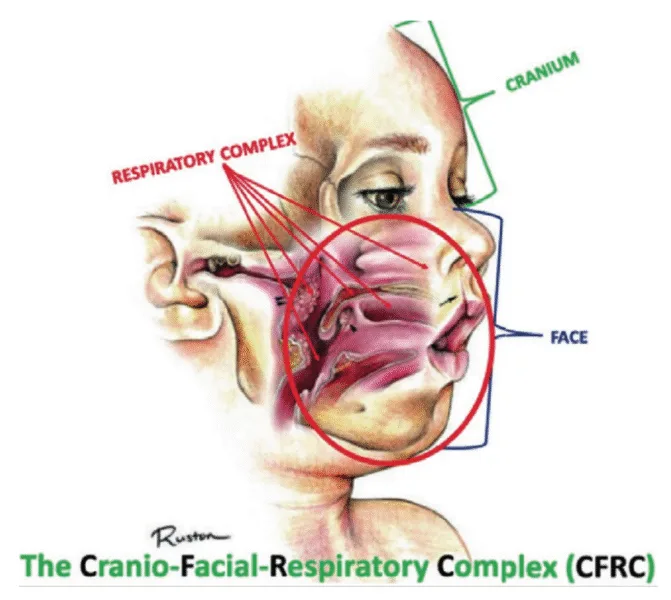
A pediatric-patient dedicated Sleep Medicine laboratory setting is difficult or impossible to find, setting aside what is considered the diagnostic gold standard, overnight PSG. Most screening questionnaires can be valuable as SRBD morbidity assessment tools and reliable for predicting increased risk. They are based solely upon identifying SRBD behavioral phenotypes known to be associated with sub-optimal sleep hygiene (e.g., snoring, teeth grinding/bruxism, excessive bodily movements). The Sleep Clinical Record (SCR)15 is an exception because it relies on not only behavioral morbidity traits, but also some physical morbidity traits such as constrictive/retrusive and retrognathic jaw maldevelopments,16 which are known to be associated comorbidities with SRBD.17 Most of these physical traits can be classified as malocclusion phenotypes and generally are located within the inter-connected craniofacial respiratory complex (CFRC)18 (Fig. 1) which was foreshadowed by Dr. LeRoy Johnson in the opening paragraph of this review: ‘The face has evolved with the functions of mastication and respiration.’- L.J. 1921.
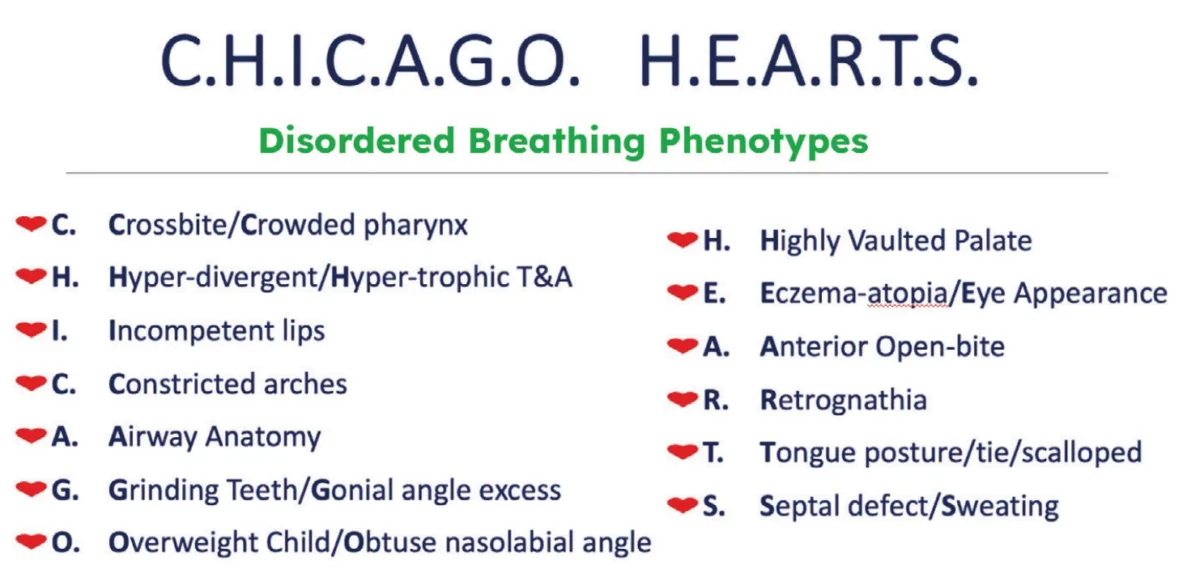
While the SCR goes further than most other screening assessment tools towards identification of some CFRC/SRBD co-morbidities, it is limited in its comprehensiveness. Ideally, in addition to screening for birth/perinatal history risk factors, such as pre-term birth,19,20 clinicians should have validated screening tools for identifying behavioral comorbidity traits, and for identification of physical risk phenotypes of the CFRC. The CHICAGO HEARTS screening tool combines these survey areas. (Fig. 2).

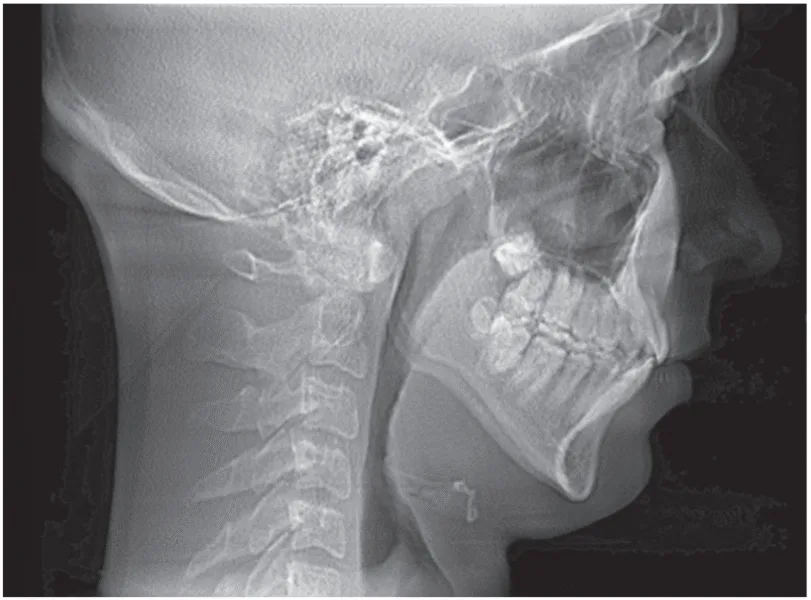

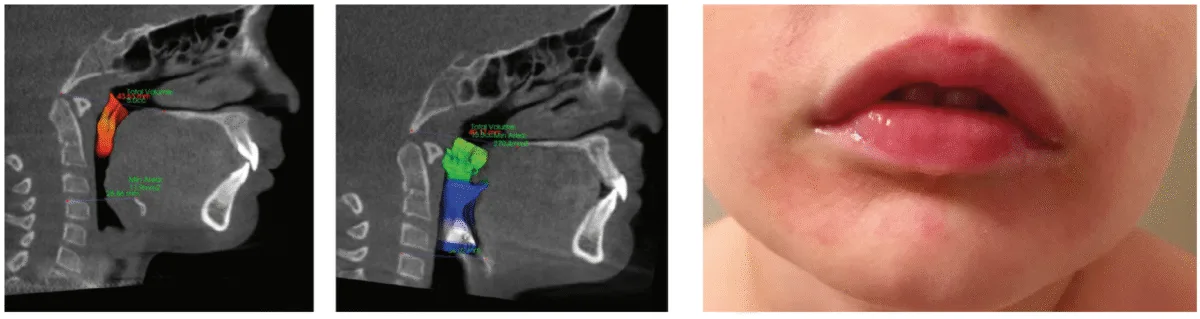
In a lecture held in 2018 at Boston University entitled ‘Sleep Disordered Breathing/Obstructive Sleep Apnea Symposium’,21 a new screening tool called C.H.I.C.A.G.O. H.E.A.R.T.S. (C.H.) had been introduced as potentially becoming the first validated screening device specifically designed to identify CFRC physical traits that can often be comorbid with SRBD. Several of these traits are listed within the C.H. acronym (Fig. 2). For instance, under the first letter ‘C’ are listed: Crossbite 22,23 Fig. 3 and Crowded Pharynx;24,25 ‘H’: Hyper-divergent growth (Fig. 4),<>16 Hypertrophic tonsils and/or adenoids;26,27 ‘I’: Incompetent lips;28 ‘C’: Constricted arches (Fig. 5);23,29,30 ‘A’: Airway anatomy (Fig. 6);22,31 ‘G’: Grinding teeth (bruxism)32 and Gonial angle excess;33 ‘O’: Overweight child34 and Obtuse nose-lip angle( NLA);35 ‘H’: Highly-vaulted palate;36 ‘E’: Ezcema-atopia37 and Eye appearance-venous pooling38 and scleral show;39 ‘A’: Anterior open-bite (Fig. 8):40 ‘R’: Retrognathia (Fig. 9) (mandible16 and/or maxilla);41 ‘T’: Tongue posture,42 tie (tether),43,44 scalloping;45 ‘S’: Septal deviation46 and night Sweats (diaphoresis).47

Interdisciplinary Communication and Shared Learning Opportunities
There is no single provider who can treat all aspects of a child’s developing airway, so it is necessary for every provider to communicate with other professionals. While dentists are used to working with specialist colleagues, merely filling out a referral form is inadequate. Multi-provider patient care requires sharing of critical information without the benefit of commonly-accessible health records or free clinical time to dig through dense reports in order to find the next step in the child’s health care plan. To achieve a balance between not-enough and too-much data in the report, agreements setting appropriate communication expectations are the way to go.
George Bernard Shaw famously said: “The single biggest problem in communication is the illusion that it has taken place.” This unfortunate truism exists in medicine today. The doctor who first identifies the child at risk has the primary duty to guide the patient (and their family) through the diagnostic and treatment option process. This is best done by contacting the child’s pediatrician (or family PCP) for medical status updates, share concerns, and work out the next steps to be taken. As the dentist opens the discussion, they must keep in mind that the physician likely had about 2 hours of instruction on all aspects of sleep-related topics during residency. The dentist is well-served to recall the paucity of the topic in their own professional school and approach colleagues first with curiosity about their comfort with the evaluation and management of children with airway problems. Assuming other providers are well-aware of the subject might lead to defensiveness or other impediments to helpful exchange of information. The physician might appreciate the informed dentist helping them navigate unfamiliar territory; when done respectfully, the dentist-physician relationship improves.
A strategy that has worked well in several dental offices known to the author is for the dentist to reach out to providers important for diagnosing, treating, and managing SRBD in the community and initiate small-group meetings to establish common ground. Each provider (dentist, pediatrician, otolaryngologist, children’s sleep specialist, orthodontist, myofunctional therapist, school nurse – the list can include many health care professionals) is invited to share with the group their perspective and engage with others about how their expertise is valuable. Dentists, unlike physicians, are used to study clubs and other mutual-learning environments. Clarity of purpose and diplomacy in presenting the opportunity to providers who might question the need for such an effort is the first challenge. Once the group is assembled, before diving into the details, a ‘safe environment’ must be created so participants feel free to share their strengths and weaknesses. If the dentist is adept at convening and leading meetings, the first gathering should go well; another option would be to invite someone with facilitation skills to help with initial agreements. Like first impressions, the startup meeting sets the tone for ongoing group dynamics, where questions arise, beliefs are challenged, and discussions lead to establishment of agreed-upon protocols that can be employed in many clinical situations. For those patients who fall outside the typical presentation, the relationships built in the small group enable more effective connections between providers to establish an optimum care path. Once established, the small group can be a source of much professional comradery, shared learning experiences, and great satisfaction in practice.
If a group cannot be assembled straightaway, it takes more work, but individual relationships must be fostered. The first may be for the dentist to find an airway-oriented orthodontist and like-minded otolaryngologist to talk over patient care. These doctors are the best-trained in all aspects of the craniofacial respiratory complex and this triad can form a nucleus of a preferred referral pattern. Once protocols are developed between the small group, they can be proffered to the other necessary professionals with credibility.
Summary and Conclusions
Growing awareness of the deleterious health impact of SRBD in adults has led to a sense of urgency in a variety of health fields to develop creative approaches to treatment, but that’s a subject for another essay. Another significant development over the past 10 years has been the realization that SRBD is common in children. We have learned that adenotonsillectomy, a treatment approach effective in improving sleep related respiration in many patients with SRBD, cannot be relied on as definitive treatment. Residual and recurrent SRBD after adenotonsillectomy have been demonstrated to be common,50 leading to curiosity among practitioners who care for children about why this occurs and what can be done about it. Once again, innovations emerged from collaborations between practitioners from different fields, united by their shared desire to improve the lives of children with SRBD. These innovations included the use of medications, drug induced sleep endoscopy, and non-retractive orthodontic/dentofacial orthopedic (NRO/DO) approaches to treatment. While there are still very few examples, there is growing enthusiasm about what becomes possible when dentists, otolaryngologists, and Sleep Medicine physicians collaborate. Indeed, the imperative of having practitioners from each of these fields involved in the care of any patient with SRBD is increasingly recognized in the field of sleep medicine. What is also emerging is a common recognition that beyond treating SRBD, practitioners caring for kids should set as their goal the establishment of unobstructed nasal breathing as early in life as possible. Our recognition of the complexity of SRBD, the impact a compromised airway can have on breathing during wakefulness, and evolving attitudes about what is required to make this diagnosis have led many of us who practice in this field to begin to look outside the current paradigm for potential ways to improve the lives of our patients. Naturally, the paradigm shift from surgical treatment of SRBD to multidisciplinary non-surgical or adjunctive-to-surgery efforts to optimize nasal breathing has met with some resistance. As a result, much of the research taking place in the field is focused upon measuring emerging treatment approaches against adenotonsillectomy based on polysomnography (PSG) results. The paucity of centers capable of performing PSG in children and effectively interpreting these recordings has limited our ability to learn about these questions at a large enough scale to generate a compelling basis of evidence for the need for collaboration between the medical, surgical, and dental fields. What the rediscovery of the publications reviewed in this article show is that in the late 19th-/early 20th-Century SRBD was a known entity in early childhood and was evaluated and treated by both surgical and dental collaborators.1,2,8, 47-55 Collaboration allowed patients with disordered breathing of sleep and wakefulness, primarily manifested as habitual and chronic mouth-breathing, to get the multidisciplinary care required to optimize their airways. This suggests that while research based upon PSG evidence of improved outcomes after NRO/DO and other nonsurgical treatments of SRBD in children can and must continue, we must also give systematic attention to creating collaborative environments in which dentists, otolaryngologists, and Sleep Medicine practitioners can work in concert to screen for, evaluate, and treat disordered breathing in children. Our hope is that this review will demonstrate that these collaborations are essential and inspire a growing number of practitioners from diverse fields to begin conversations about how they can remove barriers to this approach. Let’s get back to doing what was done before!
Patients who have OSA often have co-existing conditions such as malocclusions. Read this article by Maria Sokolina about how clear aligner therapy can help patients with maloclussion and SRBD. https://dentalsleeppractice.com/a-successful-case-of-combination-therapy-using-myofunctional-therapy-an-aligner-sleep-appliance-and-clear-aligners/
Author Info
 Kevin Boyd, DDS, MSc, is a board-certified pediatric dentist practicing in Chicago, IL. He is also a dental consultant in Sleep Medicine at Lurie Children’s Hospital. He is a Visiting Scholar at the University of Pennsylvania doing research in orthodontics and evolutionary biology at the Penn Museum of Archaeology and Anthropology. Prior to completing his DDS degree from Loyola University’s Chicago College of Dental Surgery in 1986, he obtained an advanced degree (MSc) in Human Nutrition and Dietetics from Michigan State University. He completed his post-graduate residency training in Pediatric Dentistry at the University of Iowa due to its reputation for providing intensive clinical and didactic learning opportunities in the areas of early childhood orthodontics/dentofacial orthopedics, and also early childhood behavior guidance management and child psychological/emotional development. Treating and preventing pediatric disease through promotion of healthy breathing and eating is his primary clinical and research interest.
Kevin Boyd, DDS, MSc, is a board-certified pediatric dentist practicing in Chicago, IL. He is also a dental consultant in Sleep Medicine at Lurie Children’s Hospital. He is a Visiting Scholar at the University of Pennsylvania doing research in orthodontics and evolutionary biology at the Penn Museum of Archaeology and Anthropology. Prior to completing his DDS degree from Loyola University’s Chicago College of Dental Surgery in 1986, he obtained an advanced degree (MSc) in Human Nutrition and Dietetics from Michigan State University. He completed his post-graduate residency training in Pediatric Dentistry at the University of Iowa due to its reputation for providing intensive clinical and didactic learning opportunities in the areas of early childhood orthodontics/dentofacial orthopedics, and also early childhood behavior guidance management and child psychological/emotional development. Treating and preventing pediatric disease through promotion of healthy breathing and eating is his primary clinical and research interest.
References
- Johnson, L. The Diagnosis of Malocclusion with Reference to Early Treatment. 1921; J Dent. Res. 3(1):v-xx.
- Bogue, E.A. New York Academy of Medicine-section of Laryngology and Rhinology. 1912;
- Cochrane, A. Effectiveness and Efficiency: Random Reflections on Health Services. 1972; Nuffield Provincial Hospitals Trust
- Buschang, P.H. An evidence-based stepwise approach to orthopedic treatment. 2023; Seminars in Orthodontics. 29(3):271-277
- Paneth, N. Assessing the Contributions of John Snow to Epidemiology 150 Years After Removal of the Broad Street Pump Handle. 2004; Epidemiology. 15(5):514.
- Bjerke, N. The Evolution Handwashing to Hand Hygiene Guidance. 2004; Crit Care Nurs Q. 27(3):295-307.
- Faraoni D, Schaefer ST. Randomized controlled trials vs. observational studies: why not just live together? BMC Anesthesiol. 2016 Oct 21;16(1):102-.
- Streptomycin treatment of pulmonary tuberculosis: a Medical Research Council investigation. BMJ 1948;2:769-82.
- Green, R. et al. Association Between Maternal Fluoride Exposure During Pregnancy and IQ Scores in Offspring in Canada. JAMA-Pediatrics. 2019;173(10):940-948.
- Cohen, S. Malocclusion and Its Far Reaching Effects. 1922; JAMA. 79(23):1895-1897.
- Baccetti, T. et al. Early dentofacial features of Class II malocclusion: A longitudinal study from the deciduous through the mixed dentition. 1997; Am J Orthod Dentofac Orthop. 111;502-509.
- Bishara, S. et al. Changes in the molar relationship between the deciduous and permanent dentitions: A longitudinal study. 1988; Am J Orthod/Dentofac. Orthoped. 93:19-28.
- https://www.ada.org/en/member-center/leadership-governance/councils-commissions-and-committees/dentistry-role-in-sleep-related-breathing-disorders# Accessed 01/16/2020
- BEARS Owens, J. A., & Dalzell, V. (2005). Use of the “BEARS” sleep screening tool in a pediatric residents’ community clinic: a pilot study. Sleep Medicine, 6(1), 63–69.
- Chervin, R.D. et al. Pediatric Sleep Questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. 2000; Sleep Medicine 1:21-32.
- Chervin, R. et al. Pediatric Sleep Questionnaire: Prediction of Sleep Apnea and Outcomes. 2007; Archives of Otolaryngology – Head and Neck Surgery. 133(3):216-22.
- Pia-Villa, M. et al. Sleep clinical record: what differences in school and preschool children? 2016; ERJ Open Res. 2:1-8.
- Flores-Mir, C. et al. Craniofacial morphological characteristics in children with obstructive sleep apnea syndrome: A systematic review and meta-analysis. 2013; JADA. 144(3):269-277.
- Boyd KL, Sheldon SH. Sleep disorder breathing: a dental perspective. In: Principles and practice of pediatric sleep medicine. 2nd ed. Amsterdam: Elsevier Inc; 2012. p. 275–80.
- Boyd, KL and Kelly, J. Prevention and Correction of Pediatric SB/OSA and Post-T&A Relapse: A Non-Surgical Orthodontic/Dentofacial Orthopedic Approach. 2019; in: Friedman, M. and Jacobowitz, O.(eds) Sleep Apnea and Snoring 2nd ed. Elsevier Inc. p. 439-444.
- Collaco, M. Respiratory Phenotypes for Preterm Infants, Children, and Adults: Bronchopulmonary Dysplasia and More. 2018; Annals ATS 15(5):530-538.
- Ignacio, T. et al. Perinatal Risk Factors Associated with the Obstructive Sleep Apnea Syndrome in School-Aged Children Born Preterm. 2016; SLEEP. 39(4):737-742.
- Boyd, K. Structure-Function/Function-Structure of Habitual Mouth-Breathing and Malocclusion in the Primary/Early Mixed Dentitions. Paper presented at : Sleep Disordered Breathing/Obstructive Sleep Apnea Symposium, Boston University, March 10, 2018
- Fastuca, R. et al. Airway compartments volume and oxygen saturation changes after rapid maxillary expansion: A longitudinal correlation study. Angle Orthodont. 2015; 85(6):955-961.
- Galiotti A. et al. Prevalence of malocclusion in children with obstructive sleep apnoea. Orthod Craniofac. Res. 2018; 21:242–247.
- Tsuiki, S. et al. Oropharyngeal Crowding and Obesity as Predictors of Oral Appliance Treatment Response to Moderate Obstructive Sleep Apnea. CHEST. 2013; 144(2):558–563.
- Ito, E. et al. Oropharyngeal Crowding Closely Relates to Aggravation of OSA. 2016; CHEST. 150(2):346-352.
- Ballikaya E. et al. Oral health status of children with mouth breathing due to adenotonsillar hypertrophy. 2018; Int. J Ped.Otorhinol. 113:11–15.
- Oliver, OA. The Evil Effect of Adenoids and Tonsils Upon the Dental Arches. 1918; The International Journal of Orthodontia. 4(8):391-394..
- Saitoh, I. et al. An exploratory study of the factors related to mouth breathing syndrome in primary school children. 2018; Archives of Oral Biology 92:57–61.
- Pia-Villa, M. et al. Efficacy of rapid maxillary expansion in children with obstructive sleep apnea syndrome: 36 months of follow-up. 2011; Sleep Breath. 15:179–184.
- Stellzig-Eisenhauer A. and Meyer-Marcotty, P. Interaction between otorhinolaryngology and orthodontics: correlation between the nasopharyngeal airway and the craniofacial complex. 2010; GMS Current Topics in Otorhinolaryngology – Head and Neck Surgery. 9:1-8.
- Major, M et al. Agreement between cone-beam computed tomography and nasendoscopy evaluations of adenoid hypertrophy. 2014; Am J Orthod./Dentofac. Orthoped. 146:451-459.
- Rouse, J. The Bruxism Triad Sleep bruxism, sleep disturbance, and sleep-related GERD. 2010; Inside Dentistry. May:32-44.
- Anderson, S. et al. Correlation between gonial angle and dynamic tongue collapse in children with snoring/sleep disordered breathing – an exploratory pilot study. 2018; J Otolaryngology – Head and Neck Surgery 47:41-46.
- Gozal, D. Obesity and Excessive Daytime Sleepiness in Prepubertal Children With Obstructive Sleep Apnea. 2009; Pediatrics. 12(1):13-18.
- Conley, S.R. et al. Facial Soft Tissue Changes Following Maxillomandibular Advancement for Treatment of Obstructive Sleep Apnea. 2007; J Oral Maxillofac Surg. 65:1332-1340.
- Guilleminault, C. et al. Death and the Naso-maxillary complex. 2012; European Journal of Pediatrics 171(9):1349-58
- Ramirez, F. et al. Association of Atopic Dermatitis With Sleep Quality in Children. 2019; JAMA Pediatrics 173(5):1-9.
- Sundelin, T. Cues of Fatigue: Effects of Sleep Deprivation on Facial Appearance 2013; Sleep. 36(9):1355-1360.
- Posnick, J. and Sami, A. Individuals With a Long Face Growth Pattern and Excess Inferior Scleral Exposure: Is There Improvement After Maxillary (Le Fort I) Advancement and Vertical Shortening? 2015; J Oral Maxillofac Surg 73:1809-1815.
- Smithpeter, J. Relapse of anterior open bites treated with orthodontic appliances with and without orofacial myofunctional therapy. 2010; Am J O Dentofac. Orthoped. 137:605-14.
- Monteiro, P. et al. Dentofacial Morphology of Mouth Breathing Children. 2002; Braz Dent J. 13(2): 129-132
- Guilleminault, C. et al. A frequent phenotype for paediatric sleep apnoea: short lingual frenulum. 2016; ERJ Open Res. 2:00043.
- Yoon, A. et al. Ankyloglossia as a risk factor for maxillary hypoplasia and soft palate elongation: A functional – morphological study. 2017; Orthod Craniofac Res. 20:237–244.
- Weiss, TM. The Association of Tongue Scalloping With Obstructive Sleep Apnea and Related Sleep Pathology. 2005; Otolaryngology–Head and Neck Surgery.133:966-971.
- Guilleminault, CG et al. Adenotonsillectomy and obstructive sleep apnea in children: A prospective survey. 2007; Otolaryngology–Head and Neck Surgery. 136:169-175.
- Hung, KS et al. Night sweats in children: prevalence and associated factors. 2012; Arch Dis Child. 97:470–473.
- Whiting GF. Mouth-breathing and its Attendant Evils. 1883; Dental Cosmos.;5(6):295–306.
- Pullen HA. Mouth-breathing. 1906; Dental Cosmos. 48(10):998–1014.
- Haskin WH. The relief of nasal obstruction by orthodontia-A plea for early recognition and correction of faulty maxillary development. 1912; Laryngoscope. 2(11):1237–60.
- Sobotky, I. Persistent Mouth Breathing Following Adenoidectomies. 1913; Boston Medical and Surgical. J 168(7):231-32.
- Bogue EA. Enlargement of the nasal sinuses in young children by orthodontia. 1909; J Am Med Assoc. 53(6):441–4.
- Bogue EA. The position of the deciduous teeth, an important diagnostic symptom. 1921; Int J Orthodon Oral Surg. 7(5):237–50.
- Bogue EA. The Relations of the Dental Arches to Pathologic Affections of the Nasopharynx and Adjacent Parts. 1907; Jour.A.M.A. 49(2):102-105.
- Weeks, MS. Relation Between Abnormal Breathing and Malocclusion. 1913; Archives Dis. Childhood. 30:46-51.
- Brown, G. The Application of Orthodontia Principles to the Prevention of Nasal Disease. 1903; Dental Cosmos. 45(10):765.