Table of Contents
Do dental laser education and proficiency certifications fail patients’ and dentists’ expectations across the globe?
by Peter Vitruk, PhD, MInstP, CPhys
In the summer of 2018, when traveling with the family on vacation in Europe, my 26-year-old daughter underwent an emergency operculectomy – excision of the inflamed (due to infection) soft tissue flap over an erupting wisdom tooth. We opted against a scalpel for fear of spreading the infection, the intra-operative bleeding, and other complications. The dental office did not have a surgical laser or electrocautery/electrosurgery available, so the dental diode it was. Fully understanding the limitations of the hot glass tip diodes for soft tissue surgery, we were choosing the lesser risk of infection while preparing for painkillers … and possibly a lot of painkillers just in case the diode was not used at its best. For three weeks following the surgery, the pain in the mornings was 10 out of 10 … This made me wonder even more about some of the diode frenectomies on infants, for whom painkillers are not an option.
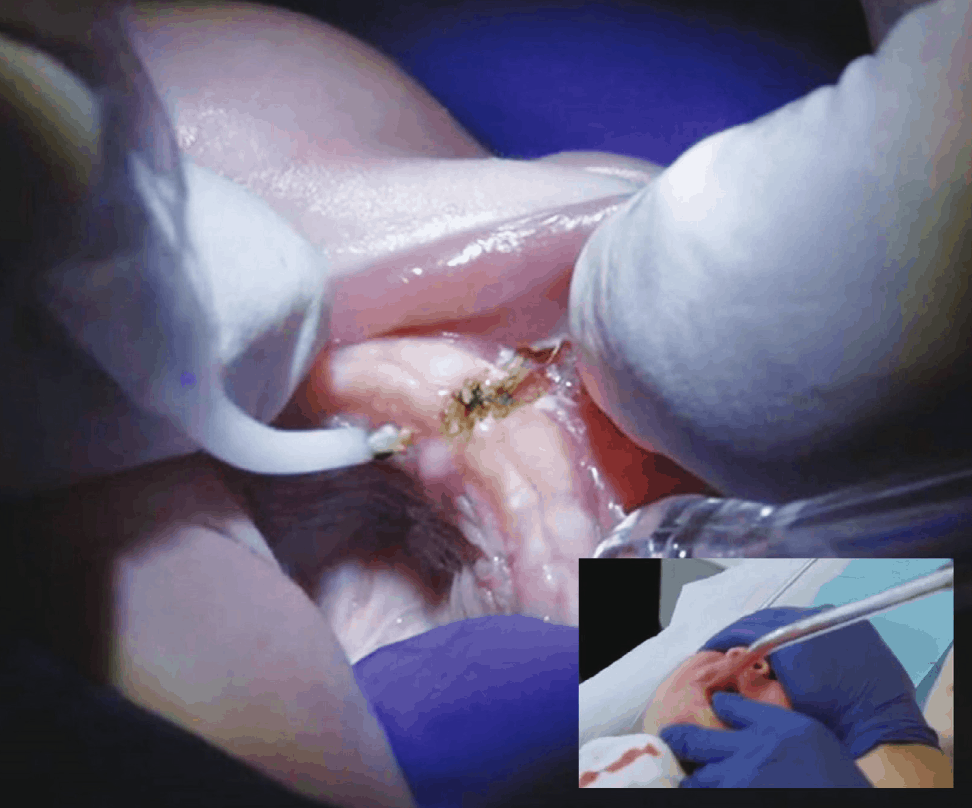
Mid-March 2019 – a video of an infant frenectomy performed with a diode’s hot glass tip was aired by the SBS TV channel in Australia.1 The images, shown in Figure 1, of the charred frenectomy site and the blood-filled suction tube are not for the faint-hearted.
In both cases above, the excisional/incisional – i.e. soft tissue cutting – diode surgeries were presented as “laser surgeries”. However, neither the excessive post-op pain, excessive tissue charring, deep thermal necrosis, or the excessive bleeding are expected during true laser surgeries performed with an appropriately configured (wavelength, pulsing and fluence) beam of laser light.2-8
So, what differentiates such diode surgeries from laser surgeries? And if the cutting diodes are indeed different from the lasers (as reviewed below), then what are the reasons that diode surgeries continue to be confused for laser surgeries?
Dental Diodes for Soft Tissue Cutting
Near-infrared (near-IR) diode laser light circa 1,000 nm is EXTREMELY WEAKLY ABSORBED by the soft tissue2,3 and, therefore, cannot optically (i.e. by the photons) ablate the sub-epithelial oral soft tissue. Instead, the diode laser optical energy heats up the purposely darkened (e.g. CHARRED) distal end of the fiber GLASS TIP to 500-900ºC,2 which then heats up the soft tissue through heat conduction from the hot glass tip. Then the soft tissue is burned off, on contact, with the hot charred glass tip. Unlike the non-contact surgical lasers (such as CO2 or Erbium lasers that vaporize tissue’s histological water by the photons of light3-8), soft tissue cutting diodes are contact thermal cautery devices, similar to electrocautery. The medical efficacy and the safe use of cutting diodes that require their tips “initiated” or “activated”, depends on multiple factors, such as:2
- User’s technique and skill in charring the glass tip, e.g. with burnt ink or cork;
- User’s hand speed and tip-tissue contact duration;
- Degradation of the glass tip’s char, which reduces tip temperature and leads to mechanical tearing (cutting) of the tissue by the glass tip’s sharp edges (hence the risk of bleeding);
- Biocompatibility and sterility of the char that’s produced by burned ink or cork when applying the hot tip to the soft tissue;
- Biocompatibility of the hot glass and its cladding materials at 500–900 degrees Celsius operating temperatures when applying the hot tip to the soft tissue;
- Risk of thermal gradient-induced fractures and disintegration (into patient’s mouth) of the hot glass tip.
The only proper way to use any hot tip cautery device for incisions with minimal depth of the thermal necrosis on surgical margins is to minimize its contact time with the tissue.8 A complicating factor when using a diode for cutting, is a halo of high intensity infrared light that surrounds the (partially “initiated” i.e. partially transparent) tip inside the soft tissue and contributes to even deeper thermal necrosis.8 Furthermore, when the hot charred tip is dragged through the soft tissue, the friction strips the char off the glass tip.9 Without the char, the glass tip cools down and may mechanically tear (cut) the tissue – which results in bleeding. Therefore, it is not surprising that both excessive thermal necrosis and excessive bleeding can occur during diode surgeries.
The hot tip cautery technique is very different from the true laser surgery technique. Without knowing that a cutting diode is a hot glass tip cautery device, it is challenging for anyone to properly use it.
Therefore, diode frenectomies performed with a hot glass tips should not be confused with, and should not be referred to, as laser frenectomies.
Deficiencies in Laser Dentistry Education Materials
Unfortunately, many of high profile laser dentistry education resources, for instance from the Academy of Laser Dentistry,10 do not describe soft tissue cutting near-IR diodes as hot glass tip cautery, and the important properties of hot tip cutting diodes are not taught in most of laser dentistry textbooks.11 For instance, the “Laser Fundamentals” chapter in the “Principles and Practice of Laser Dentistry” textbook11 never mentions that dental diode wavelengths cannot optically – with photons – cut the oral soft tissue; and it also fails to mention that dental soft tissue cutting diodes are hot glass tip cautery devices. Furthermore, the absorption coefficients by the soft tissue for the Near-IR diode laser wavelengths are often greatly exaggerated.10,11 Not surprisingly, dentists across the globe are misled and confused about the proper techniques of using dental diodes for soft tissue incisions.
It is encouraging, however, that some of the newest laser dentistry textbooks12 recognize and point out the necessity of charring of diode’s glass tips for soft tissue cutting.
The much-needed change, driven by the science of the laser-tissue interaction2-9 and by the prominent leaders in continuing dental education,13 is finally coming to laser dentistry education.
Deficiencies of Dental Laser Proficiency “Certifications”
The proliferation of Dental Laser Proficiency “Certification” courses (e.g., from the American Board of Laser Surgery)14 further confuses and misleads dentists through the false sense of being “certified”, and yet not being fully trained to treat live patients with lasers.
The one or two day laser dentistry classes are great as introduction to lasers. Typically, a majority of attendees at such “certification” courses have never owned or even used a laser. Such courses cannot make an attendee to become proficient in laser dentistry or laser surgery if such attendee has never treated a live patient with a laser. A 5-10-minute-long hands-on laser practice on pig jaws, typical for “certification” courses, cannot make one proficient in laser dentistry or surgery. Arguably, “Dental Laser Proficiency Certification” should include the proof of live patient laser treatment competence and excellence by the providers, and not just an over-the-weekend class.
Summary
In order to meet patients’ and dentists’ expectations across the globe, the standards for dental laser proficiency certification and the quality of the dental laser education resources must be elevated. Laser dentistry education must be based on Science of laser-tissue interaction.2
The soft tissue absorption spectra clearly define diode’s near-infrared wavelengths as non-ablative.2-9 If used for cutting, the near-infrared diodes are turned into the hot glass tip cautery devices, which operate vastly different from a true laser beam surgical device.2,3,8,9,12 Without knowing that a cutting diode is a hot glass tip cautery device, it is challenging for anyone to properly use it. Therefore, diode frenectomies performed with hot glass tips should not be confused with, and should not be referred to, as laser frenectomies.
Peter Vitruk, PhD, and Dr. Martin Kaplan take a closer look at laser frenectomies in their article “10,600-nm CO2 laser frenectomies in pediatric patients with compromised airway and swallowing: case reports” here.